Across healthcare, we are seeing a meaningful shift in how care teams are organized, supported, and connected. Virtual nursing, remote observation, centralized monitoring, digital patient engagement, and AI-assisted workflows are no longer distant concepts. These connected care strategies have arrived and have created a shift in the paradigm of care delivery.
That is an encouraging evolution. But as a nurse, I would offer one important caution: connected care transformation is not primarily a technology project.
Technology enables the work, but people determine whether it succeeds.
Organizations seeing the most meaningful progress are not simply installing cameras, devices, or dashboards. They’re taking the time to prepare their teams, redesign workflows, define roles, engage frontline staff, and build the trust required for new models of care to take hold. In many ways, the preparation is more important than the technical implementation.
April Saathoff, DNP, RN, NI-BC, CPHIMS, Vice President and Chief Nursing Information Officer at Johns Hopkins Health System, who rolled out a Virtual Nursing program of 202 beds on 7 units across 4 hospitals, captured the gravity of upfront preparation at the recent ATA Nexus event:
“Successful virtual nursing begins well before go-live. While technology installation and solution design are important, critical work lies in bringing multidisciplinary teams together to co-design workflows that are practical and aligned with existing clinical practice. Engaging staff early ensures that key considerations are not overlooked and fosters a deeper understanding of how the model supports their work. As a result, adoption shifts from an exclusive focus on change management to shared ownership of care. These early discussions about the future state create a strong foundation for the project, guiding decisions and enabling a thoughtful design that ultimately improves patient outcomes.”
When health systems begin planning for virtual nursing, the natural tendency is to focus first on the technical questions: What devices will go in the room? How will the platform integrate with the EHR? Where will the virtual team sit? How will calls be routed?
Those are all important questions. But they are not the first questions I would ask.
I would start with: What work are we trying to redesign? What burden are we trying to relieve? What does the bedside team need most? How will patients and families experience this model? How will we know whether it is working?
Virtual nursing introduces new ways for bedside and remote team members to collaborate. That requires clarity. Bedside nurses need to understand what the virtual nurse will do, what remains at the bedside, how handoffs will happen, how escalation will work, and how the model will help rather than interrupt their day. Virtual nurses need defined competencies, clear workflows, and a shared understanding of how they support care continuity, quality, education, admissions, documentation, and more.
That means involving bedside nurses, virtual nurses, nurse leaders, educators, informaticists, physicians, ancillary teams, IT, quality, patient experience, and even patients and families in the design process. Staff concerns should be addressed early. Workflow gaps should be surfaced before go-live. Training should include not only how to use the technology, but how to communicate and collaborate across care spaces, and how to preserve the human connection that sits at the heart of nursing.
I often remind teams that adoption is emotional before it is operational. Nurses need to trust the model. That trust is built through preparation.
Readiness must include measurement
Preparedness also means knowing what success looks like before the program begins.
Virtual care leaders should identify the metrics that matter most to their organization, capture baseline data, and train teams on how their work contributes to measurable impact. That may include admission and discharge cycle times, documentation burden, patient education completion, interpreter use, fall rates, pressure injury prevention, HCAHPS domains, staff satisfaction, nurse vacancy, agency spend, or time returned to bedside teams.
This measurement mindset is especially important for nursing. Too often, nursing work is deeply valuable but inconsistently quantified. Virtual nursing gives us an opportunity to better capture the impact of nurse-led interventions, not only in terms of efficiency, but in quality, safety, experience, and workforce sustainability.
The next generation needs exposure before practice
There is growing interest in enhancing workforce preparedness for digital health before clinicians are hired as well.
As connected care becomes embedded in clinical practice, nursing and medical education are evolving as well to give students earlier exposure to the tools, workflows, and care models they will encounter in modern healthcare environments.
Tomorrow’s clinicians will practice in settings where the hospital room may include digital whiteboards, smart TVs, in-room cameras, voice-activated workflows, virtual interpreters, remote family engagement, ambient documentation support, and AI-assists. They will need to know how to use these tools safely and ethically. But just as importantly, they will need to know how to communicate through them, evaluate the information they generate, protect patient privacy, recognize bias or limitations in AI-supported workflows, and maintain clinical judgment in a digitally enabled environment.
This is why digital health education belongs in nursing and medical programs, not as an elective novelty, but as a practical component of clinical readiness. Nursing schools are increasingly incorporating virtual care scenarios and communication training into simulation labs to build AI literacy, remote assessment skills, and data-informed escalation protocols.
Preparing people is the path to sustainable transformation
Connected care offers tremendous promise. It can extend scarce resources, improve patient and family communication, support safer workflows, reduce burden on bedside teams through more flexible models of care.
But sustainable transformation will not come from technology alone.
It will come from the thoughtful preparation of the people using it. It will come from engaging clinicians early, designing workflows around real operational needs, training teams with intention, measuring impact, and preparing the next generation of healthcare professionals for a more connected clinical environment.
The future of care will be digital, but it must remain deeply human. Our responsibility as healthcare leaders is to prepare the workforce for both.
Six Signals from NRHA 2026: What Rural Health Leaders Are Watching
Author: Scott Andrus, Senior Vice President of Sales, Caregility
At this year’s National Rural Health Association annual conference, transformation funding shared the stage with a much harder question: what happens next?
At this year’s National Rural Health Association (NRHA) annual conference, Rural Health Transformation Program (RHTP) funding came up in nearly every session. But the more interesting story was what the conversations were really about underneath.
Across keynotes, breakouts, and the conversations in hallways and over coffee, a recurring theme surfaced: people are not just thinking about how to win RHTP awards. They’re thinking about what their state, network, and hospital look like five years after the funding cycle closes. RHTP was repeatedly described as a once-in-a-lifetime opportunity, but the room treated it less as a finish line and more as a starting gun.
Six signals from the conference:
1. Rural Health as Economic Infrastructure
The most consistent theme of the conference was that rural health is no longer being discussed solely as a clinical access challenge. Speaker after speaker connected rural hospital viability to jobs, tax revenue, school enrollment, and community stability. The reminder that one in five Americans lives in a rural community came up repeatedly, often alongside the observation that when a hospital closes, the impact extends well beyond patient care.
Leaders framing rural transformation as an economic resilience instead of a one-off initiative are finding it easier to engage state legislatures and community stakeholders who don’t typically sit at the healthcare table. The funding follows the narrative.
2. States are the Strategic Control Point
RHTP is federal money, but the design, prioritization, and distribution decisions are happening at the state level. State Offices of Rural Health, ORHT structures, and state project offices will be the practical decision-makers for the next several years.
There’s no single playbook. The approach varies state-by-state in terms of who owns the plan, which rural associations hold influence, and which rural facilities, FQHCs, EMS agencies, and networks are positioned as priority participants. The states that move first are likely to set patterns that the rest of the country borrows from.
3. EMS is the Crisis No One Can Ignore
One of the most striking data points from the conference was that 47 of 50 states reported active initiatives to address EMS challenges. A speaker from Nevada described ambulance transport distances of up to 160 miles in frontier areas. Rural EMS is not simply a transport issue; it is an access infrastructure question that touches emergency care, transfers, behavioral health response, maternal care, and trauma.
Virtually enabled EMS – including remote triage before transport, specialty consultation during long transport windows, and advanced practice provider support in the field – was repeatedly named as one of the highest-potential use cases for RHTP funding. For organizations that have historically focused on inpatient telehealth, this is a meaningful expansion of where connected care is heading.
4. Cooperative networks are emerging as a sustainability template
One of the more energizing case studies came from North Dakota. The state has 23 Critical Access Hospitals, and several speakers described a cooperative network structure with equal membership, shared services, and aggregated capabilities. Although low-volume rural providers often lack the scale to support modern care delivery individually, they can gain meaningful leverage collectively.
For technology partners, payers, and policy leaders, the implication is significant. Network-level engagement is likely to be more scalable than facility-by-facility relationships. Cooperative and clinically integrated network models also create the scale needed to support shared analytics, workforce strategies, and value-based care participation in ways that individual rural hospitals struggle to do alone.
5. Workforce is the Universal Constraint
Workforce came up in every state-level conversation, and it was rarely framed simply as a recruitment problem. Broader clinical staffing challenges include an aging rural nursing workforce, fragile primary care pipelines, behavioral health shortages, EMS staffing instability, and the persistent challenge of attracting caregivers to communities where there may be limited or no spouse-employment options or specialty schools.
The more interesting conversations were about workforce redesign rather than workforce supply. Virtual nursing, remote specialty coverage, shared staffing across networks, mobile simulation training, and AI-assisted documentation are increasingly being treated as core workforce strategy, not as technology projects that happen to have workforce benefits.
6. Telehealth is Ubiquitous, but the Framing Has Changed
Telehealth came up in nearly every state-level discussion, alongside behavioral health and workforce. But there was also a cautionary signal worth noting. At least one state association suggested telehealth might be deferred to a future phase of RHTP planning in their state, with workforce and EMS prioritized first.
The takeaway is not that telehealth is losing momentum. It is that generic telehealth (“more virtual visits”) is no longer a compelling pitch. The conversations that landed were the ones tied to specific operational outcomes such as keeping fragile service lines viable, supporting maternal and behavioral health access, enabling rural EMS, extending specialty coverage, and supporting value-based care performance. Telehealth as connected care infrastructure resonates. Telehealth as a standalone product category increasingly does not.
Thinking Past RHTP Funding
The NRHA conference reinforced that rural healthcare is at a critical inflection point. RHTP is a once-in-a-lifetime opportunity to stabilize, redesign, and modernize rural healthcare delivery, but the dominant message was clear: rural health transformation cannot simply fund legacy models. It must create sustainable access, strengthen the rural workforce, enable innovative care models, and improve preventive and value-based care.
The months between now and December, when most state award decisions are expected, will establish the foundation for a multi-year redesign of how rural care is delivered, financed, and sustained. The organizations that win in this cycle will not be the ones with the slickest technology implementations. They will be the ones that engage state ecosystems early, partner with cooperative networks, design programs around workforce realities, and build operating models that have a credible path to surviving the end of the grant period.
Frame of Reference: The AI Problem & What it Actually Takes to Solve It
Author: Kedar Ganta, Chief Product, Technology, and AI Officer, Caregility
In my post on Navigating Polanyi’s Paradox, I argued that AI cannot replace tacit knowledge but can augment it. A camera can see but does not understand. This raises the natural question of what we can do to bridge the gap.
Many of us are familiar with the Abbott and Costello routine, Who’s on First, that made audiences laugh for nearly a century.
What makes it work is not that either man is wrong. Both are reasoning perfectly. The problem is that they are operating from entirely different frames of reference, and neither knows it.
The same dynamic is now showing up in AI systems.
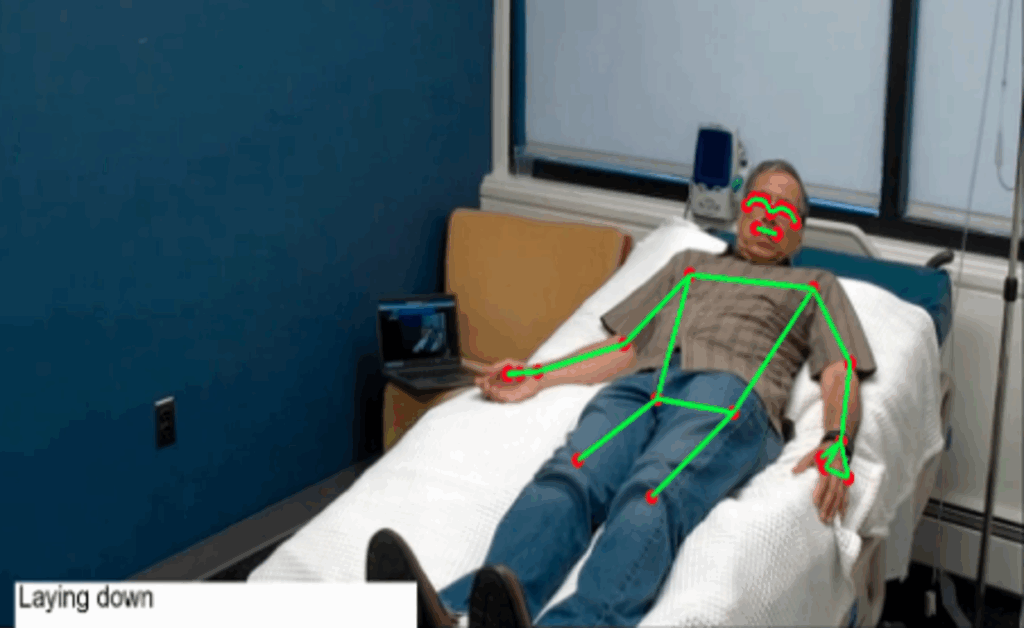
For instance, suppose a patient hasn’t moved in fourteen minutes. Computer Vision system generates a fall alert. The clinical staff respond, only to see the patient in the restroom.
The system reasoned correctly within its own frame of reference. The problem is that the frame is now decoupled from the world it was supposed to describe. The camera saw no presence. It had no concept of where the patient had gone. It processed the signal correctly but interpreted it incorrectly.
We have spent an incredible amount of time asking whether AI makes errors.
We have spent considerably less time examining something more subtle and consequential.
AI may be reasoning correctly from a frame of reference it cannot fully share with us.
And when it fails, we often end up diagnosing the wrong problem.
This is not a hallucination problem. It is not a bias problem, at least not in the conventional sense.
It is a frame of reference problem. It may be the most underestimated design challenge for leaders building AI products.
Signals Are Not Meaning
A frame of reference error occurs when a measurement or observation is made from the wrong reference point, producing an interpretation that is internally consistent but factually wrong in the world where it has to operate.
This idea shows up across different domains.
In physics, motion is always relative. A person walking inside a moving train appears slow relative to the train, and fast relative to someone standing on the platform. Neither observer is wrong. But confuse the frames, and your conclusion becomes meaningless.
In Computer Vision, a camera detects a position in pixel coordinates: an x and y in image space. But the real question is spatial: is the patient in bed, on the floor, out of the room?
If the camera shifts slightly, for example, during cleaning, or if its tilt changes, the same pixel coordinates no longer correspond to the same physical reality.
The AI system continues to reason correctly within its frame of reference. But that frame has changed from the reality it is supposed to describe. The result is false alerts, missed events, and an erosion of trust in the AI system that is very difficult to diagnose if you don’t know what you are looking for.
Large language models operate at a more abstract level of the same condition. They have processed more human-described experiences than any individual will encounter in a lifetime. The model generates a fluent, confident account of situations it has never experienced. The words are not attached to anything felt. Follow the chain of reasoning far enough, and it never quite touches reality.
The Inverse of Polanyi
Michael Polanyi observed that we know more than we can tell. The experienced machinist, craftsman, or clinician cannot fully articulate what guides their hands. Tacit knowledge, the kind which is embedded in the body and accumulated through years of practice, cannot be explained in simple language.
AI inverts this paradox almost perfectly.
AI can tell more than it will ever know. It produces a detailed and confident account of situations it has never seen, decisions it has never made, and consequences it will never bear.
Polanyi showed us that language falls short of describing experience. The ‘frame of reference’ problem shows us that language, no matter how sophisticated, cannot replace experience.
This is the paradox your organization is building on.
This is not a flaw to be patched.
It is a structural condition of the technology. Not a model failure. Not a data quality problem, but rather a frame of reference misalignment.
It shapes what AI can and cannot be trusted to do, regardless of benchmark performance. This is a fundamental condition in which AI operates. The question is what we do about it.
Where Leaders are Already Feeling This
You probably haven’t labelled it a ‘frame of reference’ problem. You may have called it something else.
The AI tools that you are using aced different benchmarks and confused your users at scale – that was a frame misalignment. We have evaluated our Computer Vision in our AI lab. In other words, it was evaluated by people whose context matches its output. When the Computer Vision is deployed into context where that alignment was gone, it processed every signal available to it in a specific context.
Stop Designing as If the Gap Does Not Exist
The response to ‘frame of reference’ problems is not a smarter model. It is a more honest system design that treats reference frame alignment as a first-class engineering problem rather than an assumption.
Here is what we built to address the problem.
Make the frame explicit. In the spatial orientation, we looked at the field of view and transformed the camera sensor output before drawing inferences. In physics, this is a coordinate transformation. In Computer Vision, this is calibration and homography. Using Homographic transformation, we handled the 2D mapping from image plane to floor plane, accounting for camera height, tilts, and resolution.
Build the translation layer. We created a mechanism for moving between different frames of reference by combining multiple sensing modalities. Consider a scenario where radar and computer vision operate together to monitor occupancy. Radar detects presence in room coordinates, while computer vision detects a person in image coordinates.
In a restroom, for example, radar can confirm continued presence where camera coverage is intentionally absent for privacy reasons. When these signals are properly aligned, they tell a coherent and actionable understanding of the situation. When they are not aligned, the opposite happens. The systems are effectively speaking different spatial languages, with no translation between them. The result is noise with alerts that lack context, which erodes clinical confidence and increases alarm fatigue.
Recalibrate proactively. Frames drift as the camera shifts, or something else happens. Using computer vision, we take operational control to automatically recalibrate the camera position and restore an accurate field of view before any interpretation.
This is not an algorithm problem. It is a systems problem of establishing a shared canonical frame into which every sensor output is transformed before any inference is attempted.
Those who navigate this well will not be the ones who wait for that question to be resolved. They will be the ones who design explicitly for the gap, who treat reference frame alignment as infrastructure rather than assumption, and who recognize that the most dangerous AI failure mode is not the one that looks like an error.
The Shift
We are moving from model-centric AI to system-centric AI. In this next phase, success will not be defined by who has the most advanced model or the largest dataset.
Success will be defined by who can align signals across modalities, ground outputs in real-world context, and operate reliably within the correct frame of reference
AI does not fail simply because it lacks intelligence.
It fails because it interprets the world without sharing our frame of reference. Bridging that gap is not just a technical challenge. It is a product challenge and a systems challenge.
And solving it is what will separate AI that works in controlled demonstrations from AI that works reliably in the real world.
What’s New: Caregility January-March 2026 Update
Author: Kedar Ganta, Chief Product, Technology, and AI Officer, Caregility
Following my December 2025 update, I received feedback from a hospital system that had deployed our Virtual Observation program across multiple units:
“We still have blind spots we cannot ignore – especially in spaces where cameras simply can’t go.“ That comment captures the tension we face in healthcare: how do we extend patient safety everywhere it’s needed while still respecting dignity and privacy?
One innovation I’m particularly excited about showcasing is our Radar-Based Monitoring – a silent observer in spaces where cameras don’t belong, such as restrooms and other privacy-sensitive areas. It is designed to act as a second layer of awareness, expanding monitoring capabilities while preserving patient dignity.
We’re also expanding what’s possible with sound captured directly from devices in patient rooms. This includes voice commands that allow patients and staff to trigger hands-free actions, monitor decibel levels for a more comfortable healing environment, and ambient documentation captured directly at the point of care.
We’ll also feature the AI Playback alongside our CUBE AI Server – both designed for operational realities of real-world hospital environments. We will be demonstrating these practical innovations, built responsibly, and designed to improve care in real hospital environments.
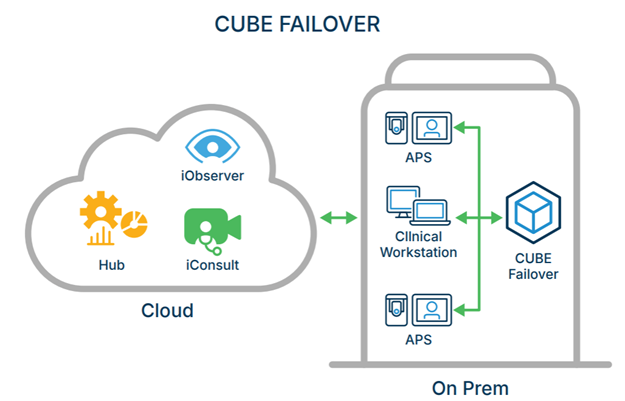
CUBE: Your Continuity Server
We’re introducing the CUBE server – Caregility Cloud Continuity Server. It’s designed for the scenario no one wants to think about, but everyone needs to prepare for: what happens when a disaster strikes?
When a hurricane hits, when a ransomware attack locks down your network, when a major cybersecurity incident cuts off access beyond your hospital network walls, CUBE keeps your virtual care running.
It’s a local failover that maintains care delivery continuity even when everything outside your four walls is disrupted. The financial and clinical impact of losing virtual care during a crisis is significant. CUBE is designed to eliminate that risk. We also offer CUBE AI server, a version that processes large AI workloads locally, extending our edge-first architecture.
January Platform Release
In January, we delivered significant workflow, intelligence, and compliance enhancements across iObserver, iConsult, our endpoints, and Control Hub.
iObserver Brings Smarter Monitoring Workflows
You can now download HL7 audit logs that capture names, encounter details, dates and times – the kind of record keeping that compliance teams need, and clinical teams increasingly rely on.
When clinicians and observers join the same session, we now share camera position signals between them. If an observer zooms to 5x or switches to 40x, clinicians can see which view is active to prevent confusion.
Session-transfer intelligence now preserves privacy mode settings and recording status when handing off a patient from one observer to another. These states persist through a successful transfer, ensuring continuity during handovers and shift changes.
iConsult Inpatient Consultation Enhancements
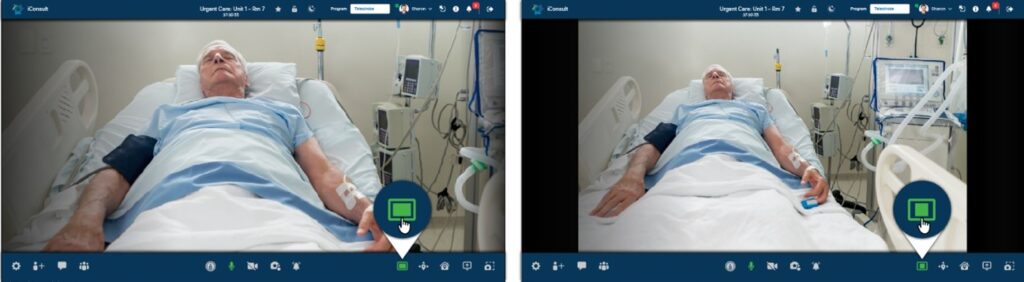
iConsult calls now feature default blurred background for better privacy during consultations.
We now support ‘second spotlight’ to keep the patient visible to ASL interpreters, allowing them to maintain visual contact for hearing impaired participants.
iConsult calls can be placed directly from Epic Mobile Apps (Rover, Canto, Haiku), with better interpreter lookup for language assistance.
Devices now display a busy message when occupied with another call, while maintaining auto-answer capabilities on bedside patient apps.
Control Hub Gets Better Visibility
Our command center is looking sharper with advanced reports (beta) for clinical notification.
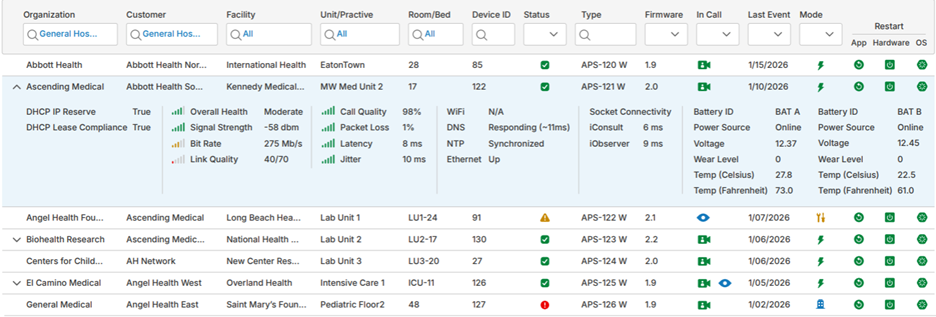
Administrators can now view device connectivity status while devices are on standby and during active use, helping teams proactively monitor performance and manage their device fleet more effectively.
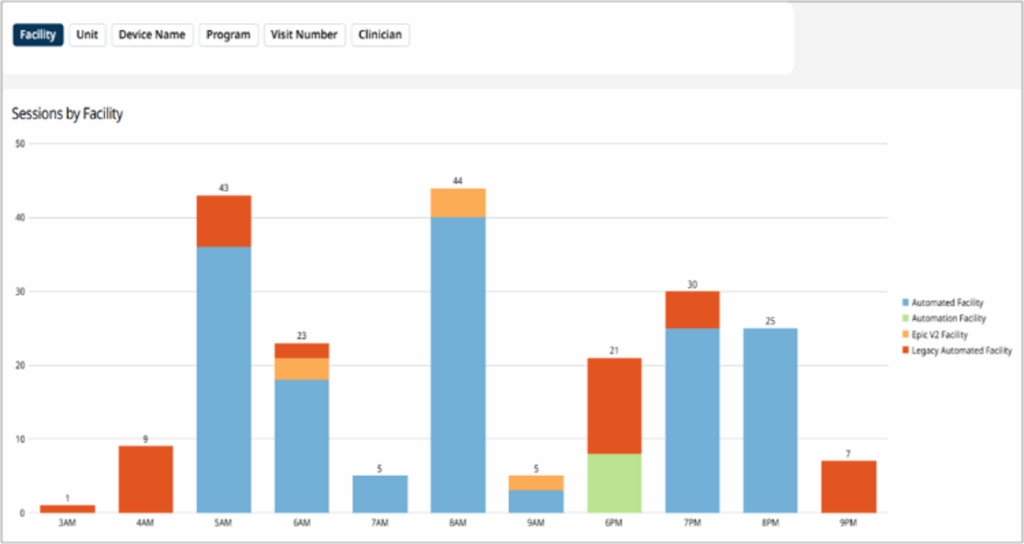
Track calls that are answered on the first push versus those requiring multiple attempts, with average response times for benchmarking. Drill down by program, call type, organization level, or individual user.
With up to 24 months of data visualization, you’ll gain insights you need to make informed operational decisions.
See which camera endpoints and tablets are online, offline, in a call, or inactive – visibility that helps teams manage endpoints and reduce disruptions across care environments.
Administrators can now better manage and plan the replacement of their Caregility carts’ batteries with battery health stats.
Endpoints Get Even Smarter
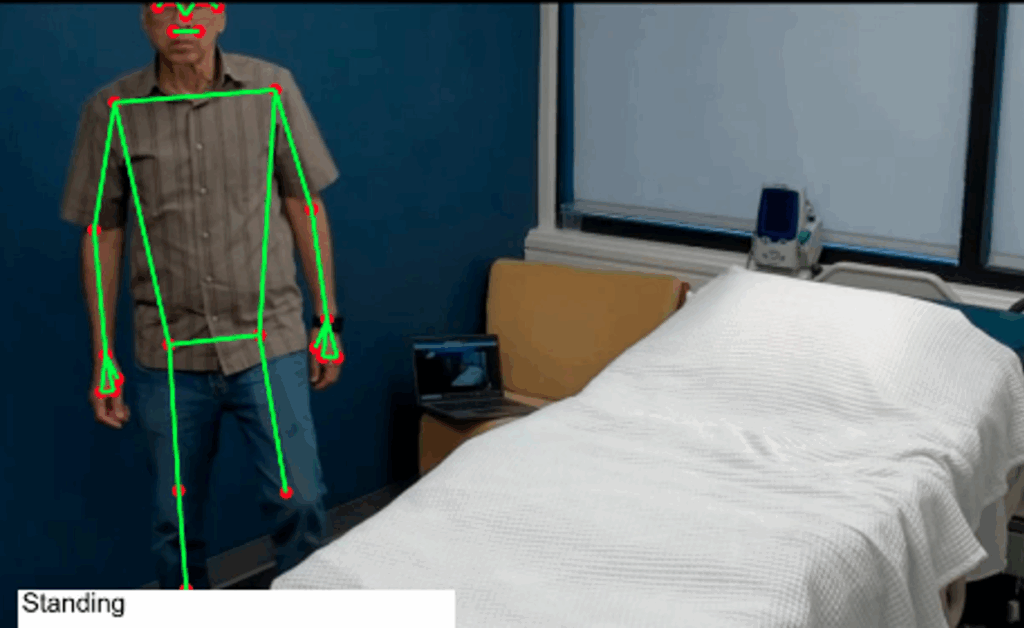
Our AI-augmented observation continues to evolve. The platform uses computer vision to detect when patients are standing, sitting, or lying in bed, capturing mobility signals that matter to clinicians.
We also applied computer vision to solve a common operational problem. When cleaning protocols require physical camera adjustments, cameras can lose their home position. Our latest release uses computer vision AI to quietly instruct camera endpoints to automatically resync to the privacy bookmark position without distracting the patient. This is the kind of practical intelligence that makes our endpoints truly smart.
Our approach to AI is deliberate, embedding intelligence that reduces friction without increasing cognitive load.
Continuing Our Focus on Intelligent Expansion
If you missed it, check out our recent announcement about AI-enhanced unlimited patient monitoring in iCare Coordinator. That adds unlimited continuous monitoring across patient rooms, limited only by individual choice. This means nurse managers now have a unified, real-time view of all rooms in a unit, giving them situational awareness. The vision is to bring AI into the mix to help caregivers act faster and smarter every day.
A Year of Momentum: Caregility’s Biggest Moments of 2025
Healthcare delivery continues to evolve as organizations look for new ways to support clinicians, improve operational efficiency, and deliver high-quality care across settings. Virtual care has become an essential part of that transformation—shifting from isolated use cases to enterprise-wide strategies that support teams at scale.
Throughout 2025, we continued to expand our Connected Care platform, partnerships, and capabilities to help health systems operationalize connected care. From new product launches and analytics tools to global expansion and deeper integrations, the year reflected steady progress toward more coordinated, data-driven, and scalable virtual care models.
Below are the 10 key milestones that shaped Caregility’s journey in 2025.
2. Launch of LOOP (Lens on Organizational Performance) Introduced our Lens on Organizational Performance (LOOP), a new analytics framework designed to help health systems quantify the operational, workforce, and financial impact of virtual care programs.
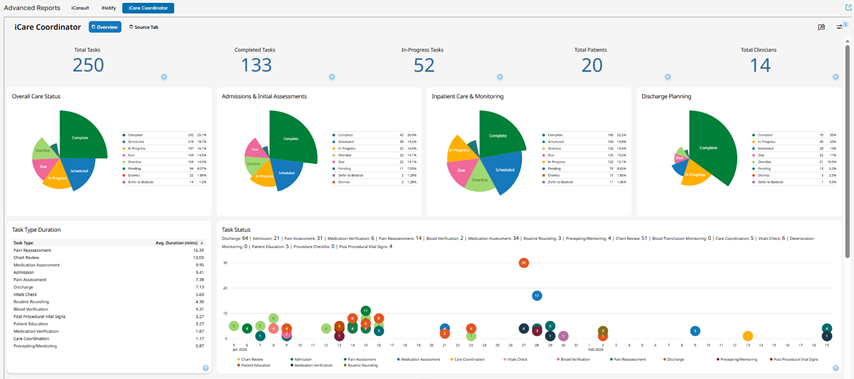
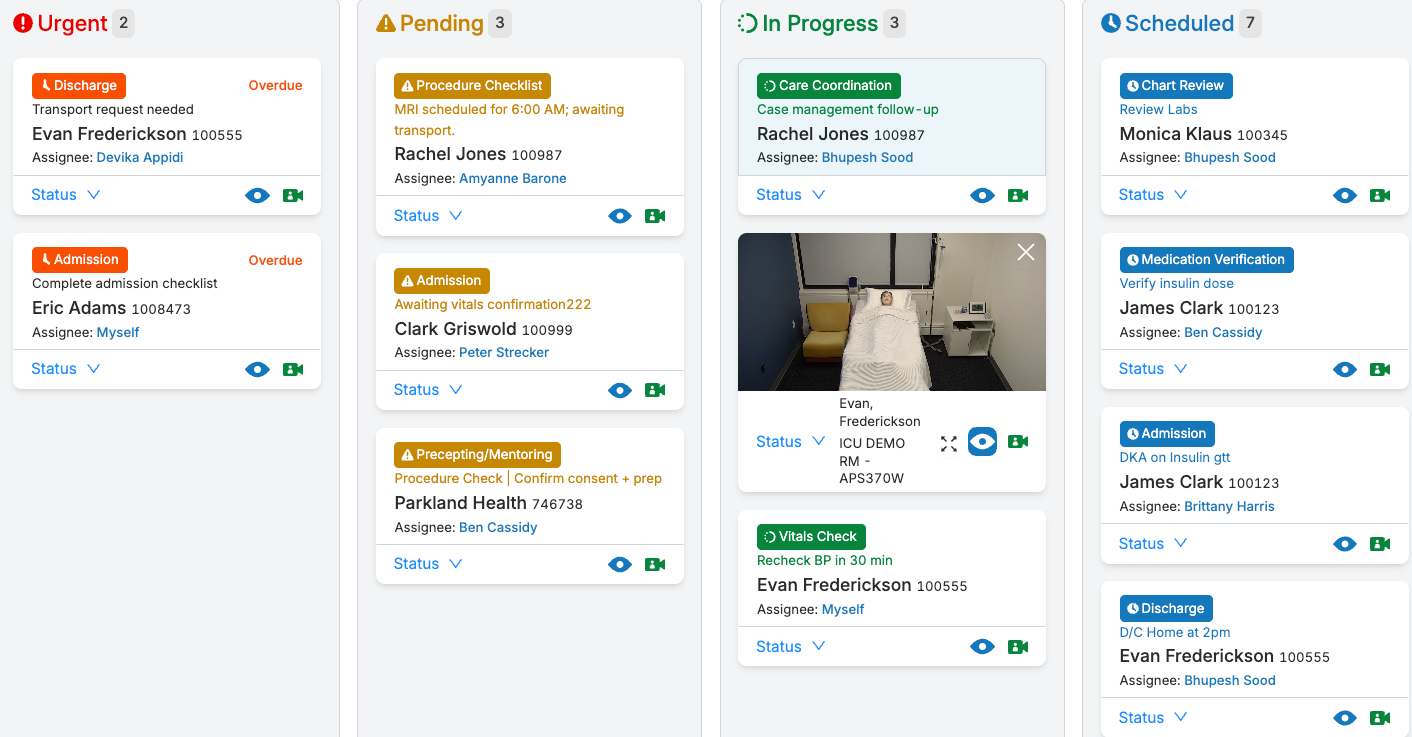
3. Launch of iCare Coordinator At HIMSS 2025, we launched iCare Coordinator – a centralized command hub that brings together virtual care workflows, task management, AI alerts, and bedside support requests into a single, streamlined dashboard.
5. Expanded Global Reach and International Partnerships Expanded our global footprint with new partners and deployments across Japan, Australia, the Middle East, Canada, and other international markets.
6. Epic Toolbox Designation for Inpatient Virtual Care Achieved designation in Epic’s Toolbox for Inpatient Virtual Care, reflecting deep integration with Epic workflows including CAL, ECAL, and Bedside TV.
8. Joint Research Initiative with Nagoya University Hospital Launched a research collaboration in Japan to explore AI-enabled virtual care models tailored to local healthcare needs and workforce challenges.
9. Significant Platform Enhancements Throughout 2025 Across 2025, Caregility released major platform updates, including Control Hub, interoperability upgrades, backend scalability improvements, expanded AI features (ambient listening, augmented observation), and accessibility enhancements.
10. Hosted a Successful Inaugural Customer Connect Summit Our customer community convened on Inova’s campus to share knowledge and ideas with speakers from Microsoft, Mayo, Johns Hopkins, Geisinger, and more!
Looking Ahead to 2026
As virtual care continues to evolve from isolated programs to enterprise strategies, 2025 reinforced Caregility’s role in helping health systems scale care, support clinicians, and deliver better patient experiences.
The momentum from this year sets the stage for continued innovation—and Caregility remains focused on helping connected care work in real-world clinical environments.
As December draws to a close, it’s remarkable how fast this year has passed. Time, as they say, is one of life’s true invariants. Throughout 2025, our team has advanced innovations that have reimagined how we make patient care smarter, safer, and more seamless, while keeping operational reliability at the forefront.
AI That Works Out of the Box
I clearly recall a conversation with a nurse manager who said, “We need technology that just works. We don’t have time or bandwidth to train your AI. And we certainly don’t want to worry about what data is leaving our hospital walls.” She was right, and she was far from alone.
The conversation reaffirmed what I already suspected: much of the approach to AI in healthcare was missing the mark. Many are pursuing increasingly sophisticated, cloud-based AI that requires extensive training and continuous patient data uploads.
So we built AI solutions that require no training. Our APS devices now deploy with AI that works the moment they are powered on. No lengthy setup, no configuration, and no patient data leaving the room. Once an APS is turned on in any patient room, it immediately understands: Is the patient standing, sitting, or lying down? Is there any fall risk? Are there early signs of bed sores? Has someone entered or exited the room?
Today, Caregility AI provides virtual bed rails, proactively identifies fall risks, maintains patient privacy screens, offers virtual backgrounds, detects room-based duress, responds to voice commands, and passively captures ambient clinical notes.
We deliberately kept the intelligence at the endpoint. While others ship data to the cloud – adding latency, risk, and operational complexity – we made the room itself intelligent. This breakthrough stems from our contrarian but deeply pragmatic view of AI.
Single Pane View of Care Management
Earlier this year, we introduced something our clinical stakeholders had been asking for: iCare Coordinator. It provides a true single-pane view of care management, bringing together all tasks and alerts required to manage patient care in one unified experience. This intuitive application is designed to reduce cognitive load and minimize context switching so clinical teams stay focused on what matters most: the patient. Caregility AI further augments care-related tasks by helping clinicians prioritize, anticipate, and act with greater efficiency.
In the middle of 2025, we crossed a significant milestone by completing a major platform uplift designed to support our continuous expansion and enterprise-scale growth to expand beyond 20,000 active patient rooms. This milestone establishes Caregility as the enterprise baseline for virtual care, delivering real care at scale, every day. As we add new sensors, introduce new capabilities, and continue to invest in new technologies, we move beyond traditional virtual care toward the vision of smart care. The APS device becomes a central hub for room-based intelligence that understands the context of everything happening in the room. It does not just provide video feed; it knows what’s happening and helps the care team respond in a meaningful way.
Security, Compliance, and AI Validation
This month, when we achieved ISO 27001 and 27701 certifications, it felt like validation of everything we have built – not just the technology, but also the discipline and governance behind how we build and operate. Our AI continues to perform at a high level in real-world environments. Based on data from real rooms at customer sites, accuracy rates exceed 90%. User feedback confirms low false positives, even across different patient room layouts and care settings. We continue to validate performance across different environments to ensure reliability, consistency, and actionable insights.
If you believe your facility has a unique room configuration, we encourage you to work with your Clinical Program Manager to check AI accuracy on your APS endpoints for yourself.
Other Product Updates Across the Platform
While we were crossing these milestones, we have been shipping several improvements
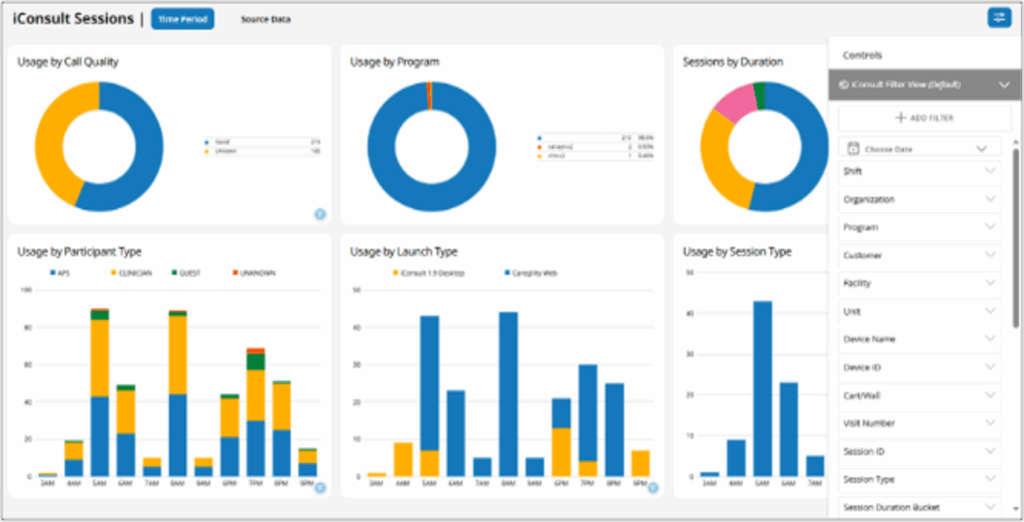
Control Hub now provides access to new reporting with rich visualizations covering device health, call quality, and participant experience. Select reports are refreshed daily and can be exported to support internal dashboards. Device monitoring has been enhanced with battery tracking, firmware status, and comprehensive audit logs across organization, facility, and unit levels. In parallel, the SSO experience has been streamlined for secure, frictionless access across the enterprise.
APS Devices now offer in-room recording capabilities that securely store content on local storage servers for compliance, safety, and quality assurance. The APS100 FlexCam and HD40 cameras have been upgraded with software for smoother, more responsive pan, tilt, and zoom camera controls. Operating system upgrades (Android 14, Ubuntu 22.04), strengthen security while expanding support for peripheral devices. These advancements enable new AI-driven capabilities, including ambient listening to support bedside nurses, augmented observation capabilities, and intelligent non-video sensors that establish patient baselines and detect environmental changes beyond video alone.
iConsult updates simplify care interactions and improve the experience for patients and families. Interpreters can now be added to iConsult calls without requiring an APS device to be connected, reducing delays and friction at the bedside. We also resolved a spotlight issue, keeping the focus where it belongs—on the patient. In addition, screen sharing has been restored for calls to mobile devices, making it easier for families to follow along during care discussions.
iNotify has been enhanced to deliver critical alerts for room-based duress and urgent notifications, ensuring staff respond immediately to safety concerns and patient needs.
iObserver has evolved into a powerful monitoring hub with AI-driven alerts that track multiple patients using virtual bed rails. It can seamlessly share APS200 Duo and HD40 camera feeds between iObserver and iConsult sessions, enabling clinicians to conduct consultations and patient monitoring simultaneously. In addition, privacy settings and recording status now persist as monitoring sessions are transferred between observers, ensuring continuity during clinical handovers. Together, these enhancements improve situational awareness and responsiveness across the care environments.
Looking Ahead to 2026 – What’s Next
As we approach 2026, we’re expanding our global footprint while continuing to invest in transformative technologies, including Agentic AI. It is more than geography – it is about expanding what’s possible.
We’re not simply building new features; we are reimagining what it means to deliver smart, contextual care at scale.
Time may be an invariant, but what we do with it isn’t. Thank you for being part of this journey. Here’s to making every day of 2026 meaningful.
In healthcare, every detail matters – a few extra decibels can disturb a patient’s rest, or an extra click can add to the clinician’s burden. This July, we’ve released several enhancements that bring us closer to building a more inclusive and intelligent connected platform.
Designing for Everyone with a Focus on Accessibility
We looked at our platform and asked ourselves the question: What more can we do to support every user? This means designing for everyone across different abilities, languages, cognitive needs, and preferences.
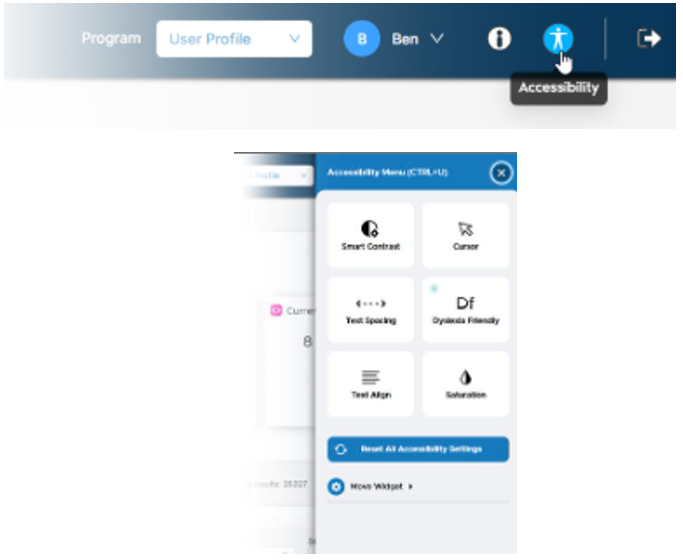
In this release, we’ve introduced a new Accessibility Widget in the Global Header for both Control Hub and iCare Coordinator. This small but meaningful addition allows users to personalize their experience with features like adjusting smart contrast, dyslexia-friendly fonts, adjustable text spacing, and cursor enhancements for better visual clarity. It’s one of the many steps in building a more inclusive platform. We are actively seeking your input to shape what comes next so everyone can navigate through our platform with ease, comfort, and confidence.
Clarity in the Control Hub
As your organization grows, so does the need to delegate access securely to manage operations. In this release, we’ve introduced a Read-Only Admin Role, allowing your system administrators to grant view-only access to certain key users. These users can now view and export data without the risk of making changes. To complement this, we are providing Bulk Program Association, enabling user admins to assign users to programs through a simple CSV import. It’s a small change that helps streamline onboarding and reduces friction in daily account management.
Device uptime and visibility continue to be a top priority for administrators. That’s why APS device endpoints now show new status indicators, giving administrators better diagnostics and real-time visibility into device uptime and activity. We are continuing to enhance device monitoring across different hierarchy levels in the upcoming release.
Intelligent Endpoints
Our APS endpoints are at the heart of every observation, call, and alert. We are evolving our endpoints into something more – an anchor in the patient room to power a more connected and intelligent ecosystem. In this release, we are making major updates to future-proof APS endpoints with OS upgrades to Android 14 and Ubuntu 22.04 for improved performance and security. We are expanding hardware compatibility with PDI, RCS, LG, and Samsung IPTV models to support two-way video calls, and to support USB peripheral devices like stethoscopes and video scopes for remote patient assessment. These changes will support emerging technologies and extend their value as a cornerstone of connected care delivery.
Sensing, Seeing, and Augmenting with AI
Our AI journey is well underway. We’re enabling various capabilities like Ambient Listening to detect distress signals in real time, Augmented Observation to monitor patient movement and behavior patterns, and Ambient Documentation to make clinical note-taking smarter. In our deployment of AI technology at some sites as part of our Early Field Trials, our computer vision technology is already showing promising results around accuracy rates. With each update, our AI becomes more deeply embedded into workflows, helping capabilities become more integrated into care delivery.
A Better Virtual Experience
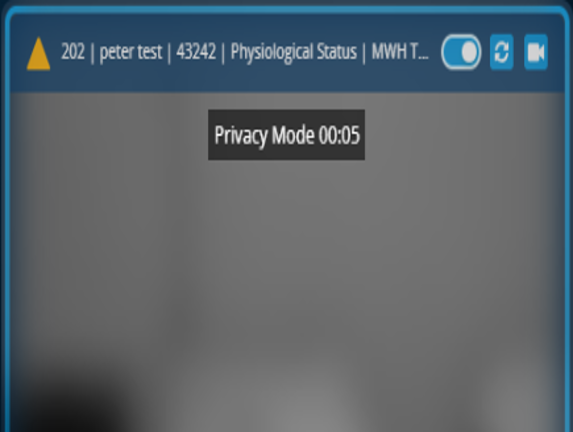
This month, we’ve refined virtual consultations to be more seamless and engaging. Users can now enjoy a full-screen view, adjustable camera widget sizes, and integrated Propio interpreter services – all directly within the call experience. On mobile, we have optimized the interface by removing unwanted cross messages to make better use of screen space. Meanwhile, the iObserver application now includes key updates such as Privacy mode with screen blurring and expanded dashboard access for greater visibility and user control.
Our continued investment in human-centered platform design – from enhancing accessibility to advancing device intelligence and AI-powered experiences – reflects our commitment to building a platform that evolves with your needs and adapts to emerging technologies.
We look forward to hearing your feedback and to continuing this journey together.
Warm regards, Kedar Chief Product and Technology Officer
What’s New: Caregility May/June 2025 Update
Author: Kedar Ganta Date: June 2, 2025
As we reach the halfway point of the year, we have crossed a major milestone in our journey to support your evolving care models. Over the past few weeks, we completed an important upgrade to the Caregility Connected Care™ platform. This shift lays the foundation for faster innovation and stronger performance as we expand with you.
With the new platform foundation, we’ve moved our core backend services to a more modern and scalable architecture. You will experience a foundation that is built for enterprise-scale growth with better load times and deeper integrations between applications. Whether you are deploying our technology across a few units or hundreds of rooms, you will see the difference.
In tandem with platform upgrades, we rolled out a host of features across our product suite. These enhancements are designed to make your workflows tighter and operations smoother.
Observers often manage several patients at once, so everything counts. We made iObserver faster and easier to use by reducing login wait times. Observers can now trigger the ‘Notify’ alarm for multiple patients simultaneously while they are in a virtual session. Moreover, to keep things smooth, we enhanced the ‘Patient Successfully Added’ notification so that it fades away after a few seconds without requiring the user to click on the ‘OK’ button.
In the next release, we will continue to invest in adding additional phrases to our ‘Multilingual Phrases’ feature. We will also be expanding access for iObserver users so they can view dashboards.
Clinicians are juggling multiple priorities – managing numerous calls and staying responsive. In the recent release, we made iConsultmore customizable and polished by giving the ability to store up to 10 custom virtual backgrounds in the Control Hub. This means clinicians can select that background or setting that best suits their role, offering a personalized video presence experience. We also worked on alert fatigue by shortening the window from 4 hours to 1 hour to remove stale alerts. This helps ensure that only actionable, not outdated, alerts are shown on the screen.
In the next release, we are making full-screen mode the default view during ad hoc calls, removing those inconvenient black bars to give a more immersive experience. Additionally, to help virtual teams stay aligned – especially across shifts – we are introducing real-time visibility. This new feature will let you see which team members are currently online, enabling more confident and informed decisions when escalating or assigning alerts.
On the AI front, we introduced a new Clinical Notes feature that is designed to make ambient note taking smarter. We are currently working with a few customers to get feedback on the workflows. Your input will help reduce documentation burden and improve charting accuracy for clinicians.
At their core, our APS endpoints are more than a device. They’re powered by multiple smart sensors that provide the input our Artificial Intelligence needs to generate meaningful insights! Stay tuned – we’ll be sharing more about the AI innovation we are bringing to the platform.
As technology evolves, APS endpoints will continue to advance along with these changes. We are updating the APS Linux OS to the 3.nn version to support AI-powered innovation. The new APS version retains all existing features while laying the foundation for smarter AI-driven capabilities. With added support for 5G and Starlink, APS endpoints can be deployed on the move, making it ideal for remote care. Keep an eye out for upcoming details where we discuss new medical peripherals, including USB-compatible video scopes and stethoscopes.
We are also making important investments in accessibility. Users will be able to adjust text size and color contrast directly from the screens using a built-in accessibility widget. In parallel, we are simplifying the data export process for Admin users, making it easier to manage and support.
These updates are a broader part of our investment in making our products more human-centered, responsive, and easier to use.
Warm regards, Kedar Chief Product and Technology Officer
What’s New: Caregility March 2025 Update
by Kedar Ganta, Chief Product and Engineering Officer, Caregility
March has been incredibly engaging and marked a true milestone for us.
Fresh off the energy from HIMSS 25, where we showcased our AI innovations – including computer vision, ambient intelligence, and native clinical notes – I’m excited to share how this momentum is translating into real-world applications for you. Over the past year, we’ve accelerated AI development, delivering production-ready solutions that assist with clinical documentation, improve patient monitoring, and reduce alert fatigue. Our vision is to rethink how AI-enabled technology transforms bedside care – augmenting nurses and remote clinicians while streamlining workflows and reducing cognitive burden.
Caregility’s native computer vision for patient observation
We’ve just rolled out a significant release featuring key improvements across our platform.
Virtual Visit Enhancements
In this March release, we prioritized enhancing the day-to-day user experience by streamlining login and logout flows for clinicians and patients. Additionally, we standardized alert notifications to consistently capture the ‘Joined’ status, regardless of whether alerts originate from mobile apps on tablets (APD), or camera endpoints (APS). Looking ahead, we will continue refining these improvements, focusing on minimizing unanswered alerts and giving clinicians more control during ad hoc Consultation Calls, with the flexibility to choose between full-screen and fit-to-screen viewing modes.
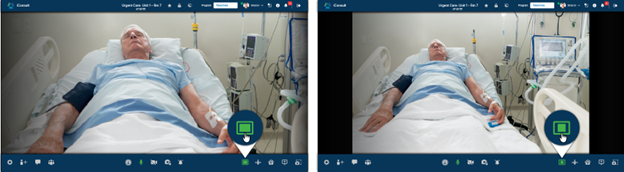
Fit-to-Screen and Full-Screen viewing options within Caregility CloudTM
Virtual Observation Enhancements
We know how important it is to have continuous patient observation. We have introduced a clear network signal strength indicator for video streams. We further enhanced Observation Workflows to simplify the transfer of observation duties between team members and make it easier to locate specific patients within large observation programs.
Patient transfer within Caregility iObserver
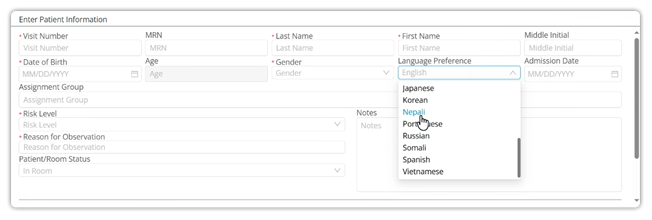
To break down language barriers, we have added support for additional languages like Nepali, Creole (Cape Verdean), and Portuguese, allowing observers to effectively engage with a wider range of patients.
New patient language preference selections within Caregility CloudTM
Platform Enhancements
Your Control Hubnow features a global header that allows you to navigate effortlessly between programs and a testing mode for quick workflow validation. We have also enhanced reporting capabilities to filter out test sessions to isolate accurate insights from real consultation and observation sessions. In the upcoming release, we are working on ways to give you more insights about the types of consultations that are happening within your program.
Telehealth Endpoint Enhancements
On camera endpoints (APS), we continue to improve resiliency. The March release includes improved connection stability between APS devices and televisions using RS-232 connections. Building on the existing compatibility with LG and Samsung TVs, we are expanding support to include IPTV devices. The APS270W now runs on the latest Caregility firmware (version 3.nn) and we plan to extend this update to other APS models. We are also enhancing the Linux and Android OS update process to ensure minimal disruption.
Excitingly, our APS devices are now compatible with Starlink and 5G cellular, opening up new possibilities for remote care. We are ready for early field trials (EFT), and your Caregility Sales contact can assist you in taking advantage of these capabilities.
We remain committed to advancing our AI roadmap and continuously enhancing our platform, and we greatly value your feedback in shaping our products. Currently, we are partnering with select customers on early field trials of computer vision and ambient documentation features. Furthermore, we are developing AI-augmented observation dashboards to get insights into patient mobility, fall risk events, and more. Thank you for your continued partnership, and we look forward to sharing further updates in the coming months.
by Kedar Ganta, Chief Product and Engineering Officer, Caregility
We are kicking off 2025 with exciting updates in our January release, including newly designed pages to elevate your experience with Caregility products.
Introducing the Control Hub
Last week, we unveiled Control Hub, your new centralized command center that allows you to:
Streamline device management with batch operations.
Easily manage and deploy the latest firmware updates across all endpoints.
Access dashboards and reports for actionable insights.
Control features across Caregility applications, endpoints, and partner integrations.
These enhancements are designed to provide a seamless, unified experience across all Caregility applications. We welcome your feedback as we continue to improve. Looking ahead, our March release will include the ability to easily switch between programs from the global header.
iConsult
Building on the positive feedback from our November 2024 release, we’ve made further enhancements:
Virtual backgrounds are now available for iConsult calls launched from third-party applications such as Epic.
Users’ background selection will now persist until manually changed or the user logs out.
Stay tuned for more iConsult updates, including a new doorbell feature to enhance privacy and user control, as well as improvements to call notification status.
iObserver
iObserverusers will notice several significant improvements:
The Program List can now be expanded into a separate full screen view, offering enlarged text and enhanced visibility to improve usability.
The new observer assignment filter streamlines and simplifies assignment management.
And there’s more to come in March! Our team is actively designing a new feature for partial transfer, enabling you to quickly send whole or partial assignments to another observer. Stay tuned for these exciting updates.
On the reporting front, the iObserver application’s Real Time Usage Monitoring now provides instant access to key application usage statistics, providing great insights such as all available endpoints by facility, average active sessions per observer, and total number of sessions.
These tools empower administrators with data to drive efficiency and make informed decisions.
ExpandingInteroperability and Connectivity
This year, we are continuing to make your Caregility APS endpoints smarter and more interoperable:
TV Integrations: APS endpoints will integrate seamlessly with LG and Samsung TVs, as well as IPC partners. We will be making APS endpoints compatible with IPTV, making in-room communication effortless. Please reach out to us for a list of supported LG and Samsung TV models.
Extended Connectivity: In 2025, Caregility APS endpoints will be compatible with Starlink and 5G networks, enabling connectivity for mobile EMS units, sea vessels, and hospitals in remote locations. With this, any APS endpoint can connect your extended medical teams to areas once thought impossible.
We are excited about what’s ahead and look forward to sharing more updates with you. Let’s connect at the upcoming ViVE and HIMSS conferences if you or your team are attending. We’d love to hear your ideas and feedback in person!
Cookie Consent
We use cookies to improve your experience on our site. By using our site, you consent to cookies.
Cookie Preferences
Manage your cookie preferences below:
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
Google Tag Manager simplifies the management of marketing tags on your website without code changes.
Name
Description
Duration
cookiePreferences
Registers cookie preferences of a user
2 years
td
Registers statistical data on users' behaviour on the website. Used for internal analytics by the website operator.
session
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_gid
ID used to identify users for 24 hours after last activity
24 hours
_ga_
ID used to identify users
2 years
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
_ga
ID used to identify users
2 years
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utma
ID used to identify users and sessions
2 years after last activity
Vimeo is a video hosting platform for high-quality content, ideal for creators and businesses to showcase their work.