Virtual Care’s Impact on Patient and Staff Experience with Christine Coriell from OhioHealth
Digital Health Frontiers – Podcast Ep. 4

Director of System Nursing Operations, OhioHealth

President and COO
Caregility
In this episode of the Digital Health Frontiers podcast, Caregility President and COO Mike Brandofino sits down with Christine Coriell, MHA, BSN, RN-BC, Director of System Nursing Operations at OhioHealth, to explore virtual care’s impact on patients and staff experience. Christine, who has extensive experience in nursing leadership, shares insights into OhioHealth’s innovative virtual care initiatives, including their Virtual Nurse program, designed to enhance patient care and alleviate the pressures on clinical staff.
Mike and Christine delve into the challenges and successes of implementing virtual acute care programs, the strategies OhioHealth uses to maintain patient satisfaction in a virtual care environment, and the critical role that experienced nurses play in mentoring newer staff. They also discuss the future of inpatient care settings, touching on the potential of AI and technology to further transform patient care delivery. Tune in to learn how OhioHealth is pioneering new approaches in virtual care to support both patients and staff experience.
Read the Transcript
Welcome to Digital Health Frontiers, where we explore the cutting edge of healthcare technology, policy, and innovation, hosted by Mike Brandofino, President and COO of Caregility. In this episode, Mike sits down with Christine Coriell, the Director of System Nursing Operations at OhioHealth. In her role, Christine oversees strategic planning, development, and budget analysis of the health system’s centralized Flex Teams, Internal Travel Team, System Staffing Office, Virtual Patient Observation, and Virtual Nurse Program. As part of the Staffing & Capacity Logistics Team she is accountable for metric analysis, collaboration, and system support for improved patient flow and operations. In partnership with Workforce Planning and key stakeholders, Christine is also responsible for the evaluation and recommendation of various expansion efforts throughout the system. Her experience gives her keen insight into the impact that virtual care initiatives are having on patient and staff experience, which she and Mike dive into today.
Mike Brandofino:
Hi everybody. It’s Mike Brandolino with Caregility. I’m here with Christine Coriell, the Director of Nursing Operations at OhioHealth. Thank you for joining, Christine.
Coriell, Christine:
Hi Mike, thanks for having me. Happy to be here.
Brandofino:
One of the things we want to cover today is really the impact of virtual care on both the patients and the staff. Maybe we can kick it off with an overview of what OhioHealth has been doing as it relates to virtual care.
Coriell:
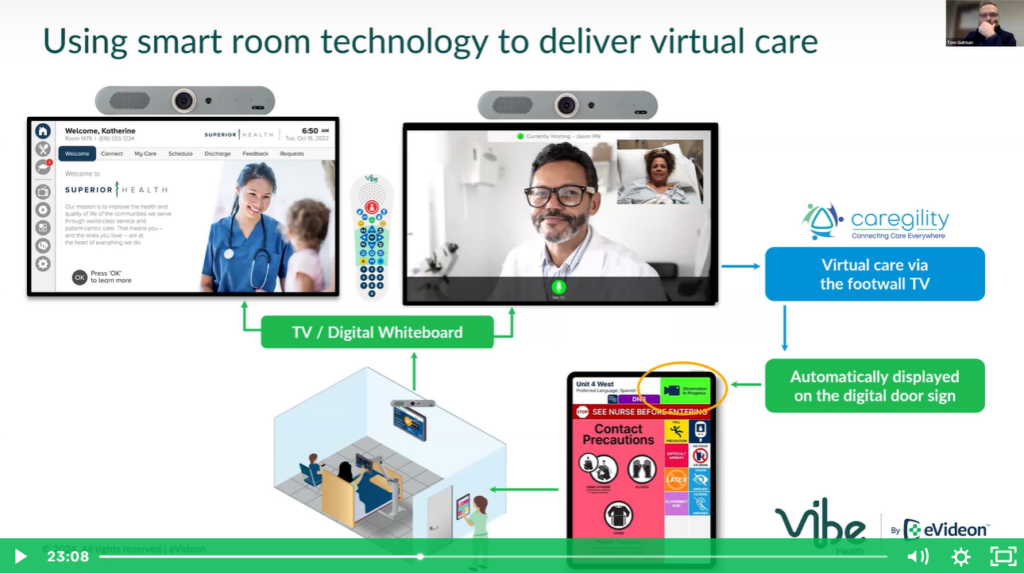
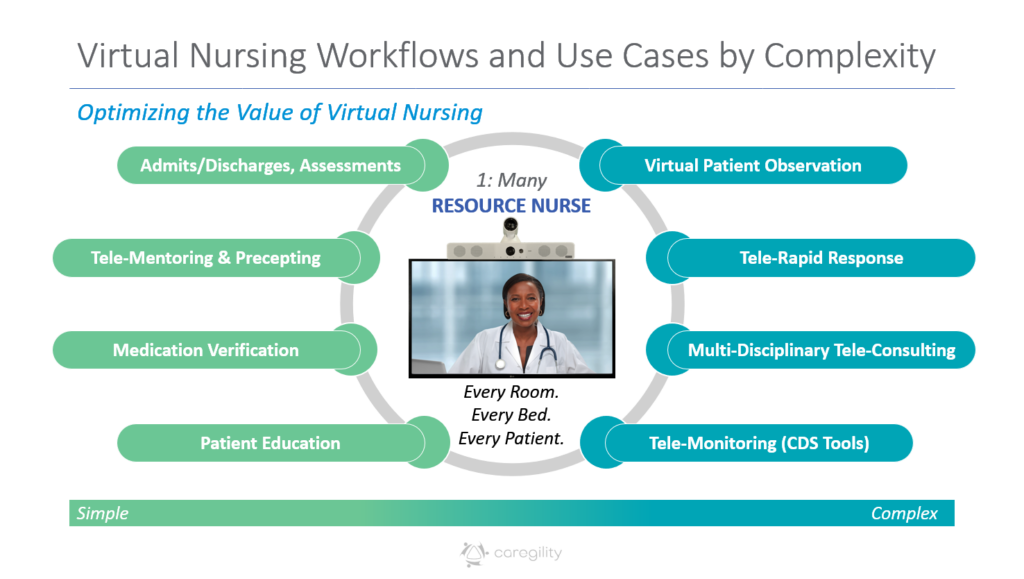
Yeah, so from a virtual care perspective, OhioHealth has many different teams, and we’ve really developed a lot of different workflows within that. For example, we have an eICU team. We also have a PSU team – that’s our Perinatal Support Unit. Neither of those teams roll up through me, but those are both teams that provide virtual services. From my structure and my accountabilities, we also have Virtual Patient Observation – so that’s those, e-sitters that sit in an administrative building to watch patients at all of our different care sites for a variety of reasons. It will exclude any patients that are there for suicide or homicidal ideations, but outside of that, we really see a wide variety of patients and reasons for having that additional set of eyes.
And then lastly, we also have our Virtual Nurse Program. So this is something that really started, gosh, almost two years ago, where we were sitting down to explore, you know, what can virtual nursing look like at OhioHealth? What do we want it to look like? What do our associates and what do our patients need this program to look like? So, we did a pilot program for about 9 or 10 months and then last December, December of 2023, is when we did go live with this program. Currently, we have it at one of our care sites. We started that program with this new care site, so when the care site opened, day one is when we started with virtual nursing as well. So, it’s been a very exciting program. A lot of things we have seen change based on the needs, again, of the associates and also our patients.
Brandofino:
Sure. And speaking about patients — you know, a couple of years ago, there was a lot of talk about the depersonalization of care if you’re using virtual care. Did you focus on patient satisfaction as part of this effort?
Coriell:
Yes, we absolutely did. You know, when we think of nursing in general, it’s certainly a combination of art and science, and we really don’t want to disrupt the human touch that we have in healthcare. That’s why many of us chose to become nurses and why we want to be nurses, so we can interact with those patients. So, from a virtual nurse perspective, when we were hiring and talking with candidates, we were really looking for something that we now call “webside manner.” We know it can be hard, at times, to connect with patients and even more so when we’re over a camera. And just like you said, we don’t want to lose that touch. So, we wanted to make sure that they have that. Ultimately any program that we’re looking at at OhioHealth, we need to factor and evaluate if we want to move forward and one of those things we talked through is how will this impact patients and patient satisfaction. And, so, this program was no different.
Brandofino:
Great. So how do you measure that? Is there a formal process? Do you do end-of-stay surveys? How’s that done?
Coriell:
Yeah. To measure patient satisfaction, we certainly think through and get those evaluations from Press Ganey, from HCAHPS. We really analyzed nurse communication. Up until this point, some of it has been hard to evaluate whether it was the virtual nurse program that positively impacted that. A lot of it is anecdotal data. But what we are going to see moving forward, and I think just two weeks ago we started, now a question is going to be going to the patients that asks if they saw a virtual nurse. If they say yes, they will then be asked about the overall rating of the virtual nurse interaction or contact. So that will be feedback about their hospital experience and valuable information that we can use to better tailor this program.
OhioHealth leaders also have accountability for leader rounding. So, what that means is 100% of patients should be rounded on every single day. With that, the unit managers can get real-time feedback and have those real-time interactions, and from that, they’re able to coach and/or discuss certain things with our associates. Ultimately, we want to ensure our patients are satisfied they’re getting their questions answered. So, leader rounding can provide that real-time alteration of what needs to happen with the patient’s day.
Brandofino:
That’s great. It’s interesting – a couple of our customers have experienced a huge uptick in the [patient satisfaction] scores. Like you said, it’s kind of anecdotal, but they’re trying to create the right metrics to capture as well. What we heard from them were things like you’re not getting the pull, the soft shoulder pull that the floor nurses get, so they’re able to spend a little bit more concerted time getting to know the patient and interacting with the patient.
We heard some really great examples of nurses taking a little extra time because they heard the prognosis that the patient got, it’s unfortunate, and they spent more time. We even heard of one nurse driving in to sit with the patient for a little while. But those scores are really important. And I’m going to say the sad part because this is what I’m hearing — it’s a soft dollar gain and, unfortunately, you know, CFOs don’t necessarily care about that. But it sounds like OhioHealth does care about patient satisfaction. And does that play into it all? What’s your experience been as far as those scores?
Coriell:
Yeah, absolutely. I think it’s important to take a step back and really see, why did we want to do the virtual nurse program in the first place? So, we had specific problems to solve when we think about nursing in general, not only in Ohio, but nationwide, We know we have a lot of staffing shortages that will really just increase over the next few years. And with that, we’re also seeing nurses with a lot less experience. So, with our virtual nurse program, we were specific on what we were looking for with those nurses.
For our program specifically, the average amount of tenure with those nurses is 12 years and we know that can provide a lot of valuable information to the associates and also patients from an experience standpoint. We also know just in general the burnout of the clinical staff, the overwhelming first year, the amount of information nurses need to know, delayed documentation, fractured communication, and also overall workflow inefficiencies – all of that can lead to a decreased patient satisfaction.
We see in any three-month time frame we have about 1,200-1,400 patients that are seen by the Virtual Nurse Program. And again, this is just one care site right now, and even more interactions with that. When we first rolled out the program, it was a one-way street is what I like to say. So, it was the virtual nurses that had to make contact with the patients. Now the patients are able to make contact with the virtual nurse, so it’s really at their fingertips to get questions answered, to have some more of that emotional support if they need, to provide education not only to the patient, but also to the patient’s family members. And we know all of that will increase overall patient satisfaction.
Brandofino:
Have you gotten any pushback from patients on this model?
Coriell:
Well, certainly anything that’s different, we will always get some pushback. Some patients think that somebody’s watching them or they’re worried that somebody’s watching them or listening to them all the time. So, what we have done and what we’re continuing to improve on is when the patients first get hospitalized, they should understand what our program is.
So, just like another nurse physically coming into a patient room, a virtual nurse is there to provide support, just in a different way. So, we found that as long as that is described to the patient and they know what to expect, that can really reduce anybody not wanting those services. If we just act like it’s another person in the care team – because that’s what they are- we get very few patients who don’t want to have that service.
Brandofino:
Sure. Yeah, I would imagine that would be the case. So, you talked a little bit about the staffing model that you use. One of the things that we saw that, again, I don’t know if it was a planned benefit, but it certainly worked. Two things one of our other customers did – one was they cycled the floor nurse. They kept it as a team. So, they cycled the floor nurse through that Virtual Nursing Program, as well as having dedicated tele-nurses. And then, the other side benefit was that some nurses that could no longer work the floor due to physical issues were able to extend their careers and keep that knowledge in the health system for helping those less experienced nurses. Is that the same thing that you saw?
Coriell:
So, to touch on the first one, you had talked about really a hybrid model – those virtual nurses work in the virtual space and then also in the care site. Up until this point, we have not done that. However, it’s something that we’re thinking about doing. I know some other healthcare systems do it, and we also have some of our virtual nurses who have expressed interest in wanting to work in the care site. We know that will just strengthen the relationships and have a better understanding of what a patient is experiencing on the floor.
So, that’s something that we’re looking into moving forward as we open the program to other care sites. We want to do a few different things. So, we’ll keep the FTE where it is, but do we want to split the FTE, or do we want to make a second position where that nurse can work in the care site? But yes, overall we want to be able to employ that model as well.
Brandofino:
Part of that leads into this question – how is the staffing’s response to it? You know, it’s funny. I think you may know we have a CNO on staff, Wendy, and we have our own clinical team and they’re constantly reminding us, “You don’t know what the day in the life of a nurse is.” And, so, we focus our effort on workflows that support that nurse in her day-to-day life. Now with the virtual Care nurse, does it feel like someone’s checking up on them, or are they embracing the help from the tele-nurse?
Coriell:
Yeah. So that’s also part of a lot of conversations that we had to have and be very intentional about and that’s not only unit leadership, that’s also nursing directors and CNOs as well. We have to have those trusting relationships so that the nurses on the unit don’t feel like somebody is watching them as well.
Again, back to the tenure of virtual nurses – we have an average of 12 years with our associates right now. They do have a lot of valuable information that they can give, and we’ve also had some great catches with that as well. And it’s how the virtual nurse is responding and coaching with that bedside nurse that can either make that experience positive or very negative. So, if they approach it in a way of, “I want to help you and assist you,” which is what we expect, we’ve seen that be positive. But that’s not, you know, without some of the challenges that we’ve had and having to talk through the bedside nurse’s understanding that the impact is not that somebody is watching over you because you’re doing things incorrectly. It’s another set of eyes, and as long as we can keep the patient at the focus of our care, which is what we do, and bring it back to the patient and patient safety, we can have those positive conversations.
Brandofino:
And I think you mentioned this earlier — I actually have a son who’s a nurse. And when he started, he was overwhelmed with what he didn’t know and I asked him the question, would that have been helpful? And he said absolutely, because they’re just so nervous about, you know, not knowing what they need to do next or just getting that extra kind of coaching. I think in a real-world situation, if it’s presented properly, it can really be beneficial to everybody, right – to the staff, but also to the patients.
Coriell:
Absolutely.
Brandofino:
So, I’m going to jump to a topic that is near and dear to everybody’s heart. Or maybe not. I’m a firm believer that AI is a technology that’s a hammer looking for a nail. We really should be focusing on the workflow and looking at what challenges are trying to be addressed and then figure out what technologies can apply.
The other thing that has come up in my mind is, OK, great. You could do it. Is it worth it? Can you act on it? Are you willing to pay for it? And I’ll give you an example. I was talking to a customer. We have access to a technology that, through dialogue between the virtual nurse and the patient, you can ascertain certain sentiment in the room. You can determine through decibels and the words being used whether the patient was being aggressive. There is also technology out there that can determine if the nurse is overly stressed. I was talking to a Chief Nursing Officer and I said, “If we could give you that data on, you know, nurses becoming overly stressed, would that be important to you?” And it was kind of a sad response and it was, “I don’t have the resources to act on that data, so giving me that data isn’t really going to help me because I can’t act on it.” Can you just comment on that concept and whether or not you’re struggling to figure out what is the right amount of data to get in order to make it useful?
Coriell:
What I’ll say first is I was laughing internally because when you were describing that, the first thing I thought of is, okay, how are we gonna be able to act on this? But I think no matter what, having that data, even if we can’t act on it at first, will better put us in a position to think in the future: What can we do? What can we change? How can we act on this?
I think no matter what, AI is going to change nursing. It’s going to change healthcare. And we need to make sure that we’re on board with that. The focus really will be on AI and how we can better care for our patients and better support our nursing associates. Predictive analytics and consumer driven health care is big right now and going to become even bigger. And without that data piece, we won’t be able to make the necessary changes.
Brandofino:
And I’m glad you responded that way because that’s our feeling too. Ultimately I I don’t think it’s going to be one thing. There’s not one silver bullet that’s going to make our lives so much better in healthcare. It’s a combination of data that we can capture from the room, data we can capture through the dialogue between the nurses and the patients, and then combining it together in a way that is something that you could look at and analyze.
So ultimately, I keep telling everybody on our team, it’s not about the technology. The technology is the easy part. It’s about what you do with the data once you get it and how you act on it, right? I think that’s really the challenge for a lot of health systems these days.
You hear about the hospital room of the future. I’ve had conversations with innovation teams and they’ll say things like, “Well, we want the family to be able to call into the room any time.” Okay, technically that’s easy, but what if the doctor is in there doing a procedure? Or what if the nurse is cleaning the patient? You don’t want the family just popping in. So, it’s more about the workflow and then fitting the technology into the workflows, at least from our perspective when we look at things.
There’s a term we use called responsible AI, and that’s really what we mean by that. Just throwing technology for technology’s sake is just not where I think people want to go. What benefit can you get out of it and is it going to add value to either the staff or the patient or both? I think those are important questions you need to ask.
Coriell:
Yeah, I agree. You mentioned AI and that would be an opportunity for us to know beforehand so we’re not disrupting a patient or not disrupting a procedure. That happens often right now, even with our virtual nurses. And that’s one thing that we’re trying to determine from a workflow standpoint, how best do we determine if we are going in and interrupting? Is that patient asleep? Is a physician in there? Is an intense conversation going on? And that’s specifically what AI can help us with as well.
Brandofino:
Sure, absolutely. Do you guys have any thoughts around what the inpatient setting is going to look like in the future? What are your hospital rooms of the future looking like?
Coriell:
You know, if we think of a few years from now, we have that one care site that has the smart room. Certainly five years from now we see that being in many of our care sites. We really see AI being a a bigger piece like we talked about, data and analytics being a bigger piece, having more technology at somebody’s fingertips to find out what’s going on, have better communication, and get better answers quicker. We know that’s what our consumers want right now. We have different pay models that will be coming up. So overall, I think five years from now what our rooms look like will be vastly different than what they do currently.
Brandofino:
Well, Christine, thank you for joining us and sharing your story with our help system customers and people out there who are interested in learning more about how programs are being run. Clearly, tele-nursing is becoming a hot-button item and many many different use cases are out there. So, I’m glad to hear about a couple of yours and the things that you considered. Thank you for joining.
Coriell:
Great. Thanks, Mike. Thanks for the opportunity.
Subscribe to Digital Health Frontiers and listen in on your favorite podcast app here.