We’re in a period of tech advancement that the World Economic Forum has dubbed the Fourth Industrial Revolution. Characterized by physical, digital, and biological worlds coming together, this period is one where tech enablement is a given, allowing us to shift our focus to finetuning the application of converging technologies.
In the Forward of “Nursing Satisfaction: What Matters Most at Work,” Ascom North America Managing Director Kelly Feist points to healthcare as a key market where you can see this revolution unfolding. Comfort with technology in healthcare picked up significantly after the pandemic, leading providers to rethink traditional care models through a new lens of digital empowerment. Today, the integration of connected devices, remote support, and AI into clinical workflows is forever changing how medical teams deliver care.
As Feist sees it, intelligent workflow technologies are more essential than ever in healthcare, due in large part to rising pressure on bedside nurses. In the Ascom nursing satisfaction survey, nurses cited increased patient loads, having to care for sicker patients, and working longer hours as drawbacks driving them away from the profession.
So, what can hospitals and health systems do to improve nurse satisfaction and retention?
Ascom notes that nurses are looking for value-adds that make the job worth doing. “This expectation can come in the form of traditional benefits like higher compensation as well as softer benefits, like greater flexibility in working hours and having mechanisms in place to make their job easier by delivering care more intelligently, efficiently, and collaboratively.”
Naturally, nurses want to be paid more for intensifying workloads, but technology is also influential in the fight for nurse talent. Almost 60% of nurses surveyed said that a hospital’s suite of technology tools was an important factor in deciding whether to take a job. Nurses want technologies to drive efficiency, give them more time with patients, and automate the capture of information into a centralized source.
Source: Ascom, Nursing Satisfaction: What Matters Most at Work
Feist highlights three takeaways from the report:
1 –Technology designed for clinical workflows consistently ranks high for addressing some of the key challenges nurses identify as negatives in their jobs. Nurses’ number one desire for workflow solutions was to eliminate redundant steps.
“Ascom identified that nurses, nurse assistants, or technicians manually measure as many as four to six vital signs per round, record each result on a chart, and then enter all of the data into the electronic health record (EHR), which could take up to three hours per shift.”
Thus the rising popularity of aware rooms and Virtual Nursing. These next-generation solutions allow bedside RNs to shift routine tasks like admissions and vitals capture to integrated devices and remote team members.
2 – Technology is increasing the time nurses directly spend with patients. The automation and remote redistribution of routine tasks are freeing up time for bedside nurses to focus on what matters to them – patient engagement.
Interestingly, virtual patient engagement channels are also offering nurses new ways to build uninterrupted relationships with patients, and supporting career extension for older, experienced nurses to continue providing patient and staff support.
3 – Technology can aid in proactive care, giving clinicians a practice “safety net” to anticipate, recognize, and intervene before a sentinel event occurs. By augmenting patient coverage with virtual eyes, ears, and sensors, care teams are alerted to potential health threats earlier, improving downstream outcomes.
The ability to manage alerts to mitigate alarm fatigue and highlight actionable cues in the ocean of new information that providers are inheriting is becoming more important.
Today, technology plays a crucial role in supporting caregivers’ ability to provide the best patient care possible. With sicker patients seeking care, limited clinician pools, and a pending surge in elderly patient populations, empowering nurses with intelligent workflow solutions not only improves nurse satisfaction today, it also modernizes care models to ensure success in the future landscape of care delivery.
How Responsible Health AI Enhances Patient Care
Artificial Intelligence (AI) is steadily becoming a part of our everyday lives. From self-driving cars to targeted social media ads, AI is revolutionizing nearly every industry. Healthcare is no exception. At Caregility, we value AI as a tool that is capable of reducing errors, supporting clinicians, and keeping patients safe. We also recognize that AI is not without its limitations and cannot replace the experience, compassion, and empathy of professional healthcare workers.
The Utilization of AI in Healthcare
The healthcare industry is no stranger to incorporating technology to deliver groundbreaking treatments while reducing costs and improving patient outcomes. Robotic surgeries, approved in 2000, are just one example of machine learning. In recent years, AI technology has become commonplace in our smartphones, watches, and other wearable devices to monitor our vital signs, ovulation cycles, cardiac rhythms, glucose levels, and sleep patterns.
The applications in development appear limitless. The following are additional examples of AI in healthcare that are already underway, or we can expect to encounter in the near future:
Enhanced genome sequencing to generate targeted treatments for genetic conditions
Reduced time and money to discover, develop, and test new drugs
Interpretation of diagnostic images to support clinical decision-making
Virtual reality technology that allows medical students to practice surgical procedures
Brain-machine interfaces to help patients with neurological difficulties communicate or function
Assistive technologies that promote safety and autonomy so aging or disabled populations can remain in their homes
These cutting-edge concepts require deep learning, a type of advanced machine learning in which AI learns and adapts from its data without human intervention. There are many layers of deep learning, where algorithms use their neural networks, which function like the human brain, to recognize patterns and predict outcomes.
AI may have the advantage of processing information much faster than the human brain, but it has yet to master the qualities of human nature and emotion. The goal is not for AI to replace the expertise of a skilled clinician but to optimize the way care teams capture and use clinical information. Still, it would be naive to underestimate the potential power of AI, given its relatively quick integration, growth, and impact. This is why we must begin the conversation about how to responsibly utilize AI without overstepping boundaries.
What is Responsible Health AI?
As advancements in AI continue, we must consider the impacts on transparency, privacy, cost, efficiency, and person-centered care. Since there is hardly anything more personal or private than our health information, we must navigate a delicate balance that keeps ethics and patient care at the forefront. According to the editorial Responsible AI in Healthcare: Opportunities, Challenges, and Best Practices, responsible AI “seeks to ensure that AI systems are developed and deployed in a manner that is ethical, fair, transparent, accountable, and beneficial to all users.”
How Caregility Uses AI to Empower Nursing Care
Nurses comprise the largest component of the healthcare workforce, with over 5.2 million active nurses nationwide. Not surprisingly, nurses spend the majority of their time in direct patient care. They perform ongoing assessments, administer medications, and complete tasks at the direction of physicians. While nurses may constantly interact with patients, they report a lack of “presence,” meaning their ability to share in the human experience with patients. Nurses frequently cite increasing documentation requirements, high-acuity workloads, and staffing shortages as factors that limit quality time with patients.
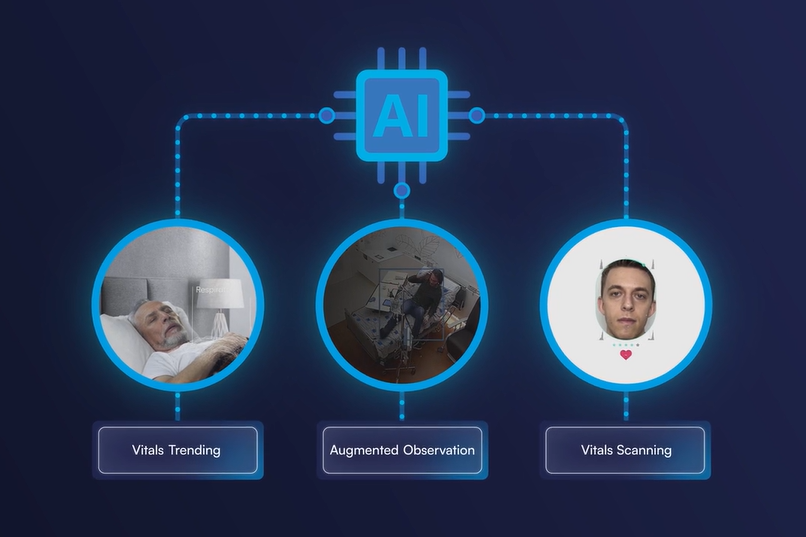
This is where Caregility’s AI capabilities make a difference. By automating certain tasks, we can afford nurses the time necessary to provide compassionate, individualized care. Here are the ways we accomplish this:
Augmented Observation. One nurse can’t be everywhere. Computer vision technology acts as an extra layer of patient safety protection to detect behaviors that could result in patient injury or adverse events, such as falls, elopement, or violence. Our iObserver application incorporates remote patient sitters to observe up to 12 patients simultaneously. With two-way audio and visual and Augmented Observation capabilities, the virtual observer can intervene rapidly by redirecting the patient or sending an alert for assistance to the bedside team.
Vitals Trending. Monitoring resting heart rate, respiratory rate, and movement is crucial in evaluating a patient’s health status. In most traditional healthcare settings, vital signs are obtained at prescribed intervals or as needed, which can delay care if the patient is deteriorating. Furthermore, frequent vital sign checks can be disruptive to the patient’s rest and recovery. With Caregility’s continuous and contactless vitals monitoring, nurses can capture patient vitals continuously, review trends over time, and receive alerts when a significant change in patient condition is identified.
Vitals Scanning. Make the most of telehealth visits with virtual vital sign scanning. Facial scanning software obtains the patient’s blood pressure, heart, and respiratory rate in less than a minute to support remote clinical evaluations. This information is useful for patient follow-up visits, as well as remote monitoring in the home setting.
AI will never replace or replicate the warm touch, listening ear, or clinical judgment of a nurse. However, Responsible Health AI can transform the healthcare landscape through enhanced patient access to care and provider collaboration. The key is to develop processes that enable clinicians to work more efficiently without creating disconnection or distrust. Caregility remains committed to this goal by integrating progressive technology and innovative workflows without sacrificing excellent human-based care.
Modernizing Mental Health Support
The numbers are sobering: It is estimated that 1 in 5 U.S. adults suffers from a mental health disorder. More than 50 million Americans carry the burden of conditions like depression, anxiety, and more. These mental health issues impact patients from all walks of life:
Young adults aged 18-25 have the highest prevalence of mental health issues (33.7%).
Mental health disorders are more frequently diagnosed among females (27.2%).
Veterans face a 50% higher risk of suicide compared to the general population.
Mental health struggles can be overwhelming and isolating, leading many to suffer in silence rather than get the care they need. Stigma and access barriers compound the suffering.
Virtual behavioral health has become an integrated part of the modern care model. The normalization of virtual options is a game-changer for patients struggling with mental health issues. Privacy, access, and convenience are a few key benefits.
Privacy: Virtual visits offer patients the same privacy and human connection as an in-person therapy session from the comfort and safety of home. Many young adults prefer the digital format for discussing sensitive issues and feel more at ease communicating through screens. Evidence suggests that this format reduces the stigma associated with seeking mental health care.
Access: Virtual mental health visits also break down geographic barriers and allow care teams to align patients with providers who share their cultural or linguistic backgrounds to promote engagement and health equity. In the face of a severe gap between staffing supply and patient demand within behavioral health, tele-psych introduces new ways to connect declining clinician pools to the growing number of patients seeking care.
Convenience: Patient interest in virtual mental health is also a reflection of the times. Familiarity with technology is more common now and a preference for more convenient, digital communication is driving usage. Providers similarly benefit from the convenience of conducting therapy sessions virtually.
Meeting Patients Where They Are
The current rate of sustained tele-psych engagement is a byproduct of smart healthcare organizations meeting their patients where they are. The success of virtual mental health services underscores the effectiveness of hybrid care models that offer patients and care teams multiple ways to engage.
By meeting patients where they are, we can help more people get the support they need without judgment or obstacles.
In a world where so much of life happens online, integrating virtual behavioral health services into care delivery just makes sense. It’s a path to more accessible, inclusive mental health care for all. A healthcare landscape that’s void of digital engagement avenues is already behind.
Learn how the Caregility iConsult application can support your behavioral health program.
Modern Patient Room Design with Peter O’Connor from Inova
Digital Health Frontiers – Podcast Ep. 3
Peter O’Connor IT Director, Eastern Region & IT Solutions Design Group, Inova
Mike Brandofino President and COO Caregility
In this episode of the Digital Health Frontiers, Caregility President and COO Mike Brandofino sits down with Peter O’Connor, Director of IT for Inova’s Eastern Region Development Program, to discuss the health system’s approach to modern patient room design. Drawing from over 30 years of experience in healthcare technology design and facility architecture, Peter shares insights into Inova’s highly collaborative approach to clinical IT enablement, which seeks to elevate patient and staff experience through hybrid care models that integrate telehealth and other technologies into bedside care.
Mike and Peter explore the integration of technology in patient care delivery, the unique task of bridging gaps between design, construction, and clinical processes, and the innovative virtual care programs that are transforming bedside care at Inova. Peter highlights the importance of culture, leadership support, and strong partnerships in driving these initiatives forward. Tune in to learn how Inova is setting new standards in healthcare delivery using technology to create seamless, patient-first experiences.
Read the Transcript
Welcome to Digital Health Frontiers, where we explore the cutting edge of healthcare technology, policy, and innovation, hosted by Mike Brandofino, President and COO of Caregility. Today Mike is joined by Peter O’Connor, the Director of IT for Inova’s Eastern Region Development Program which includes two new state-of-the-art hospital campuses totaling over 1.5 million square feet, as well as a new ambulatory facility that will include a full-service emergency room, ambulatory surgery, imaging services, a family medicine center and medical offices. Peter leverages his 33 years of technology design, implementation, and consulting experience to ensure that clinical process is enabled by technologies that meet the immediate clinical need, fit within Inova’s clinical IT ecosystem, and support the health system’s long-term digital strategy. Today Peter joins Mike to share insight into his approach to patient room design at Inova.
Mike Brandofino:
Hello everybody. Today with me, I have Peter O’Connor from Inova to talk about some of the experiences that they’ve had implementing virtual care within their health system. Hey Peter. Thank you very much for joining.
Peter O’Connor:
It’s my pleasure, Mike. Thanks for having me.
Brandofino:
Can you just describe the health system for the audience, so they get a little idea of what you guys are up to?
O’Connor:
Sure. Inova is Northern Virginia’s leading not-for-profit healthcare provider. So our mission is to provide world-class healthcare every time, every touch, to every person in every community that we have the privilege to serve. We’ve got about 20,000 team members that provide more than two million patient visits a year. We have an integrated network of five hospitals, approximately 2,000 beds, and lots of primary and specialty care practices. And interestingly enough, we’re the fourth busiest emergency room in the nation, so our hospitals are recognized with the US News and world reports. In fact, our Fairfax Hospital is the number one hospital in the DC metro area. We’re in the top 50 in neonatology, and top 20 in the nation for OBGYN.
Brandofino:
So, can you talk a little bit about your role? I think it’s a little unique, although I think some health systems are starting to put some focus around this. But can you talk a little about your focus and your position?
O’Connor:
Sure. It’s been really fantastic and it’s been a role that I really feel like my career – which is going on 33 years – I feel like the last 30 years have really prepared me for. We have a unique team at Inova for design and construction. I’d say we have a bit of a dream team. We’ve got our own engineers, architects, former contractors, & Clinical and operation experts. So, in my almost now 40 years I’ve never seen in healthcare design and construction an owner’s team with this level of experience.
So my role is pretty interesting. I bridge the gap between design and construction, IT, clinical engineering, and operations, which are typically siloed in a design process. The Inova leadership team saw an opportunity to have somebody with experience in all of those bridge the gaps and translate clinical process and what it’s going to look like in 2028 into enabling technologies and then turn that into something that can be procured and also built.
Brandofino:
You know, it’s such an interesting role and I wish more health systems would have that. So many times we’ll be talking just to the clinical side and then then when you start talking about implementing any kind of solution then either the technical side or even the facility side comes in and goes “oh, no, no -you can’t do that because of this,” or “hey, did you know there’s a lead plate in the wall next to the room that you wanted to do that Wi-Fi in?” So, I think it’s really an interesting role.
What’s it like to bridge that gap and pull those people into the same room, so to speak?
O’Connor:
It’s honestly exciting. It’s knowing that we can pull those people together in a collaborative space and brainstorm and learn from each other and really feed off of each other’s energy. It’s one of the reasons I came to Inova. I’ve had the privilege of working with lots of hospitals throughout my career in the architecture and engineering world and I’ve found that a lot of — if you could imagine folks swimming in a pool — that a lot of times it’s exactly what you said. Biomed may be going one direction, clinicians may be going in another, IT may be going another, and everyone’s swimming in a different direction. At Inova, I found that everybody was swimming in the same direction and with the same objectives and my role allows me to lift those little buoys in between the swim lanes and have everybody kind of work together and go in that same direction and see what other people are doing and leverage those experiences and come up with some really innovative solutions.
Brandofino:
How much does the patient experience fit into what you guys are trying to do?
O’Connor:
Patient experience is obviously essential. From my perspective, from a technology perspective, we want that technology to be seamless, and transparent, and to always enhance the patient and caregiver experience. When that technology becomes front-of-mind, kind of replacing healing and care front-of-mind, we’ve done something wrong. We have a tremendous responsibility to design places that heal, places that – on somebody’s worst day, whenever they feel they’ve lost all control over their environment – use technology as one of those ways to help them find some level of control and normalcy through access to information, access to education, control over their environment, access to the amazing bedside team, and make that as simple as possible for the patient. That patient experience and bringing some level of normalcy and control to a very hectic time in their world is critical for us.
Brandofino:
We spend so much time focusing, even as Caregility, on the clinician, primarily the nurse because they’re the ones using the technology the most, but we can’t forget the patient experience and what they’re going through. So that’s great that you guys have focus on that.
O’Connor:
Our IT and nursing leadership consistently remind all 650 of us IT teammates that were part of the care team. They encourage our IT team, whether you’re in leadership or you’re an analyst or you’re in the service side, to round just like the clinicians do. So, spending time on those various units gives you that real perspective of the patient and the teammate experience. Simply put, our mission is to get the right information to the right people at the right time to make great decisions.
Brandofino:
Sure. Well, stay on the clinical team. We have we have a chief nursing officer and some nurses on staff and I constantly get, “But Mike, you don’t understand what the nurse is going through in the room at the time. You’ve got to consider that.”
What insights are you getting from your clinical team as it relates to helping them in the day-in-the-life of a caregiver?
O’Connor:
We’ve had this pretty extensive design process for our new Eastern region expansion, which is two full size hospitals, full medical campuses, a Cancer Center, a specialty care center, about a million and a half square feet. So over the last two years, we’ve had thousands of hours of clinical input. We even built full-scale mock-ups of patient rooms, treatment rooms, ORs, imaging spaces, even the team stations to ensure that those designs work within that clinical workflow.
But, also, they were prepared for future technology and clinical processes. So having the clinical team come into, let’s say, a hybrid OR and they can move all the pieces around and they can mock a code or they can mock a certain procedure – gives us insight that you can’t get out of looking at a floor plan, or even can’t really get out of some of the 3D modeling. It’s just nothing beats walking into a room that’s fully constructed, and they can move things around, which is fantastic.
I would say that one of the keys to our success has been that our projects are led by a clinical team. It’s a million and a half square foot Eastern Region Expansion led by a clinical team. Heather Russell is our VP of Eastern Region Development. Eric Miller is our director of Eastern Region Development. They both have extensive clinical backgrounds. They’ve been instrumental in ensuring that the clinical voice is not only heard, but also that the clinical process is understood by everybody involved – all of us internal experts, the design construction and architecture teams. So having a construction project led by clinical operations and supported by in-house industry experts has really been our secret to success and taking that clinical voice and translating it into something that can actually be built.
Brandofino:
That’s great. Having the buy-in it is going to help. What are your biggest challenges? Sometimes the challenge is just people having an aversion to change and others are just that some of these hospitals are old or challenging to change, especially with patients in rooms and it’s kind of like changing the chassis on the car while it’s moving.
What are some of your biggest challenges?
O’Connor:
I guess from a change perspective, you’re talking about physical change from an infrastructure, but also change from a culture and thought process perspective. The good news is our CEO, Dr. Steven Jones, reminds us all – and this is in all of our Web leadership meetings, in-person leadership meetings, any time that we’re fortunate to spend with him – he reminds us to challenge the status quo and always ask why. That spirit of unrestrained curiosity has led us to either reevaluate and reconfirm current processes or quite often, it’s been the catalyst for change and to explore the why-nots and make them real. So, from a culture perspective, we are well positioned to embrace change, look for change, ask for change from the clinical level through the IT level, and design, and construction, and facilities – you name it.
But some of the challenges that we have is taking all of that that we’ve envisioned for change and documenting it well. When you’re looking at a million and a half square feet of design and you’re trying to coordinate architecture, MEP, medical equipment and technologies, security, AV, there’s a lot of moving sites or moving parts for three sites that we’re building. Traditionally projects like this, the lack of decision or direction is usually the biggest challenge. Fortunately, with our clinical leadership team on the project that’s not been a challenge really. It’s making sure that all those voices and all those hours of work and working through the clinical processes and translating that into a built environment gets documented well and gets constructed the way we expect it.
Brandofino:
That’s great. It sounds like the executive team is close to these projects and provides you that aircover that you need. That’s great to see. We’re seeing some customers who lack that kind of centralized support. You have pockets of folks fighting to try and get the attention, the funding, and get their program projects through. It seems like you guys have kind of centralized that and have the executive team providing overall air cover.
O’Connor:
We do. Our executive team, our C-level team, knows about every square foot of the new construction. Heather, being a nurse herself and a senior member of our core leadership team, that visibility and that voice – anything that we need, decisions to be made, executive direction – it’s one phone call away with Heather. And from an IT perspective, our Chief Digital Information Officer and our Chief Technology Officer are highly engaged as well as all the senior members of our networking cybersecurity infrastructure team. So, from day one, everybody’s been engaged in these projects. Throughout my career – as I’ve mentioned, I’ve worked on other projects – I haven’t seen that level of engagement. As you said, I’ve seen pockets of engagement. I don’t think I’ve ever seen the systemwide level of investment of time, energy and, direction in projects like this.
Brandofino:
That’s great. In projects this scale and size, you have multiple vendors and partners – we like to consider ourselves a partner because we’re in this for the long haul with our customers.
What are you looking for in vendors and partners as these projects progress?
O’Connor:
The scale of what we’re doing – we’re adding a million and a half square feet, two new campuses, but we also have five existing campuses and 7,000 nurses and so you’ve got a very complex existing enterprise environment and then you’re adding on to it with new construction and innovation. How do you take some of that new technology and put it into the existing environment and how do you take ideas that we want to do today and translate that into something in 2028?
What we look for are industry segment leaders that want to collaborate. Folks that are innovative themselves. They’re looking to the future. We want partners to have that same “why or why not” conversation with us and that we can have with them. It is truly that partnership of collaboration. Folks that fit into the Inova culture, that have that mindset. We need partners that are willing to work with other partners and create enhanced integrations that enable that seamless experience that I identified earlier. Without that type of collaboration and partnership – and as you said, in for the long haul – it’s not going to be easy. We’re going to be pushing and pulling on each other. But I’m a firm believer that sometimes you go through a little heat, and you create relationships. The strongest bonds are formed with heat sometimes and so you get a great partner that will get in the trenches with you and help figure this out. And then everything just seems to work out for the best. So, we’re fortunate to have wonderful, wonderful partners.
Brandofino:
That’s great. So, the buzzword right now in healthcare is Virtual Nursing. Hybrid care is another term for it. We’re actually seeing some tremendous feedback. Customer satisfaction is up. Nurse retention is up because of it in some of our health systems.
How is your organization thinking about hybrid care? Is it being embraced and are you seeing any success at it yet if you’re actually going down that path?
O’Connor:
We’ve transitioned from thinking about virtual care to living it and breathing it every day. We’ve got some innovative thought leaders from our Chief Nursing Information Officer, Maggie, our Chief Health Information Officer, Dr. Kramer, and our Senior Director of Telemedicine, Steve. We have implemented an industry-leading Virtual Nurse program, which began with some basic use cases with virtual admit and discharge, patient education, patient pain reassessment. Those use cases alone have reduced bedside time by roughly 30 minutes per nurse per shift. So, you can imagine giving 30 minutes per nurse per shift back to that bedside nurse to do the things that he or she is really, you know, in their heart, they want to do. They want to deliver bedside care, right? Not be going through a lot of things, so it’s a great use to those resources and somebody that can step in virtually and assist that patient in whatever they may need.
So now, since that’s been so successful, we’re now looking to dual consent, we’re looking to case management and wound care as additional telemedicine applications or virtual care applications. So again, expanding that footprint, that technology that we’ve invested in. You guys have been a phenomenal partner with us in doing that. So just extending that program, so all of our five sites are connected back to what we consider a very innovative high-reliability Operations Center, which is our rock where Virtual Nursing, our Central Telemetry, our Central Sitting Resource Management, our Transfer Team all operate out of the same suite on one of our floors in our corporate campus. So, you can imagine all those folks are together to make great decisions about moving patients, taking care of patients, all in that same area. We’re looking at serving 2,000 beds out of a central location. It’s been pretty innovative and it’s been open almost a year now and we’ve had nothing but tremendous feedback from our nursing teams and our patients.
Brandofino:
That’s great. We love to hear that because I think we’re getting close to a time where you could just cross out “tele” and “virtual” and it is just healthcare. It’s the way we have to deliver healthcare these days. You mentioned in the partnership, the need to be able to work together.
So how important are integrations? And from that perspective, what do you think the vision is of patient experience in Inova as you go forward?
O’Connor:
I keep on coming back to that word “transparent.” Those integrations have to be what I consider invisibly critical. And today, you know, in our personal lives, we all expect context in our alerts and how we integrate with our devices and you know the ability to delineate the noise from what’s really important and the same goes for our healthcare environment. You know the EHR gives us context, the nurse call is that patient’s lifeline, the interactive patient engagement system is that medium to provide education and information, and virtual care is that reassurance that you have a multidisciplinary team ready and available to be there whenever our patients need them, whether it’s in the patient room setting or it’s in the emergency room or it’s at home.
To your point, I think it is just healthcare. It is just a different way to meet people where they are and I think so often healthcare institutions have this mindset of “you have to come to our site, you have to be in our room.” We have two million patients that we have the privilege to serve and finding the best way possible to do that in whatever environment it needs to be is really where we need to be as an industry.
Brandofino:
Something that’s been top of mind for a lot of folks — from an ROI perspective, there’s soft-dollar ROI, there’s hard-dollar ROI – how does your CFO look at some of this? Do they consider the soft-dollar ROI as well? That patient satisfaction, the nurse satisfaction. Does that play into your ability to continue to expand these programs?
O’Connor:
Oh, absolutely. So we’re always patient-first. Fortunately, we’re a very successful not-for-profit healthcare system, and our ability to reinvest in our infrastructure, reinvest in our people, reinvest in the community and programs, we’re very blessed to be able to do that. But in order to do that, we have to be operationally efficient. We have to have the volume of patients that people want to come to Inova and want to be treated at Inova. So it does come down to those soft dollars. They are really hard to put a number on or a value on, but, again, we’re patient first so having our care team enabled with the best technology, having them to do what they do best at the bedside, having the best diagnostics and ability to intervene and deliver care – it is the most important thing to us at the end of the day. If we’re successful financially doing that it just gives us the ability to do that even more in more places to more people and have better technology.
Being a not-for-profit, private healthcare institution is a really unique thing and we’re really in control of our destiny and how we apply those resources. Our leadership team has done a wonderful job with that balance of growth and reinvesting in our infrastructure and also caring for our communities and the people who are less fortunate who can’t afford care.
Brandofino:
Clearly, you guys are a leader, and your role alone. What to me is unique in the space is really taking this seriously and putting some resources around it that really understand how to move these projects forward.
So for those health systems that are watching this, that maybe haven’t gotten started yet or had some stop/starts, can you give them a nugget of advice that can help them on their way?
O’Connor:
I think for us it’s been creating a culture where people are open and willing to listen to what doesn’t work and have the courage to ask “why not.” Having executive leadership supporting change and having partners that can collaborate and not be afraid to add a couple of destinations on the road map for us is critical. I think that the key to our success, it really does come down to – at least for me – it’s culture. It’s having an environment that lets us explore and innovate without being so adherent to recorded direction. We’re always asked the question or encouraged to ask the question “why” so for me, it’s been a culture thing.
You would think that this is all tech and innovation and being able to try different things. If you’re not in an environment that supports that, all the technology in the world is not going to help you. So it’s having the culture. Change starts with the culture.
Brandofino:
You speak my language. I always have said technology for technology’s sake is just not the way to go. If you can get the buy-in, if you have that culture that is willing to try things and fail fast, right? Not everything is going to work the first time, but if you’re willing to fail fast and try new things, I think you end up accomplishing a lot more than those who kind of wait for that perfect thing, whatever it is.
O’Connor:
Absolutely. The ability to do pilot programs and having partners willing to help us out and see what works and what doesn’t work. In an environment where you’ve you’re confident and you’ve got the confidence in your leadership team that you can try and fail and then you get up and you try again and this works. Having that environment is fantastic. We have a lot of exciting things ahead of us and we look forward to building an infrastructure where we have virtual health in every patient room. All of our new construction, we’ve got it planned and we’re working on processes and plans to move that into existing care spaces today. So you just have to position yourself and look towards the future and the future is, to your point, just healthcare. It’s not virtual health, it’s not inpatient healthcare. It’s just healthcare.
Brandofino:
Well, Peter, thank you very much for taking the time to share your experience and your story with hopefully a lot of healthcare systems that will learn from this. I really appreciate it and thanks for joining.
Examine the impact and opportunity of
the hybrid care model in inpatient settings.
Pilot Program Examples Real-World ROI How to Get Started
↓ WHAT’S INSIDE …
What can Virtual Nursing do for your healthcare organization?
Virtual Nursing helps health systems address critical issues such as nurse burnout, patient safety, and cost efficiency. This ebook offers key considerations and real-world examples to draw from as you develop your Business Case for Virtual Nursing.
Table of Contents:
What’s fueling the rise of virtual nursing?
Augmenting care teams with a Virtual Nurse component
Virtual Nursing’s reach
Virtual Nursing’s return on value
Virtual Nursing KPIs
Lessons from Virtual Nursing pioneers
Getting started with virtual nursing
Future considerations
Lee Health Virtual Nursing Case Study
Baptist Health, Caregility Expand Partnership to Enhance Patient Care
Arkansas-based health system to more than double its bedside telehealth footprint with expansion of virtual nursing, support staff, and providers
EATONTOWN, N.J. and LITTLE ROCK, Ark. (May 9, 2024) – Baptist Health and Caregility are pleased to announce an expanded partnership aimed at enhancing patient care across the Arkansas-based healthcare organization.
Baptist Health will enhance its bedside care teams by increasing its usage of Caregility intelligent telehealth devices to more than 700 bedsides system-wide, doubling the footprint of the healthcare organization’s inpatient telehealth services. The initiative adds virtual clinical resources to support in-person bedside care and help improve patient outcomes. This collaboration underscores both organizations’ commitment to leveraging technology to transform healthcare delivery and meet the evolving needs of patients and staff.
The enhanced partnership builds upon Baptist Health’s previous success with virtual admissions and discharge programs, currently supported by more than 300 wall-mounted and cart-based Caregility telehealth devices across 11 hospitals. Since partnering on virtual care services with Caregility in 2021, telehealth session volume for Baptist Health has increased from roughly 1,000 virtual visits per quarter to more than 20,000.
A Baptist Health bedside care team member welcomes a virtual clinician into the patient room using Caregility’s APS250C mobile telehealth cart.
In early 2023, Baptist Health Rehabilitation Institute successfully launched Arkansas’ first virtual nursing program to provide additional support to bedside nurses, patients and families. The program then expanded to the healing ministry’s hospitals in Stuttgart, Malvern and Heber Springs. Thanks to positive patient outcomes and feedback, Baptist Health will roll out virtual care programs on every medical and surgical floor across the organization.
As part of this expansion, Baptist Health will deploy Caregility’s new, highly advanced telehealth devices and award-winning Caregility Cloud™ virtual care platform in more than 500 additional patient rooms at the health system’s flagship hospital, Baptist Health Medical Center-Little Rock, as well as Baptist Health Medical Center-North Little Rock and Baptist Health-Fort Smith. These devices will support the expansion of virtual nursing and the rollout of virtual support staff and virtual providers in the coming months. Additionally, a centralized hub to support virtual nursing and virtual sitters has opened on the Baptist Health Medical Center-Little Rock campus.
Baptist Health will implement Caregility’s new dual-camera APS200 Duo telehealth edge devices to support the next phase of its virtual nursing rollout.
“Embracing virtual support as part of our acute care bedside support and quality strategy signifies a pivotal step forward in how we envision the future of healthcare at Baptist Health. Baptist Health first added virtual care in 2005, and we have continued to advance with the latest technology bringing us to where we are today with our partnership with Caregility. This expansion is more than an initiative; it’s a commitment to providing health equity across our state, setting new standards in patient and provider satisfaction, and furthering our mission to be the employer of choice in Arkansas.”
– Kourtney Matlock President of Baptist Health Rehabilitation Institute and system post-acute services
The partnership exponentially increases the eyes and ears able to focus on patients, reducing pressure on bedside staff by redistributing tasks that a virtual nurse or support staff can field. As a result of increased telehealth services in acute care settings, healthcare systems see significant time savings and improved throughput (the process of moving patients through the hospital system from admission to discharge). Having virtual options at the bedside appeals to patients as well, as evidenced by improved patient satisfaction ratings in early field trials.
“We are at a point where this type of care model is not an option for our health systems, it is the only way they can address staffing issues and remain competitive,” said Caregility President and COO Mike Brandofino. “This partnership with Baptist Health is a great example of how Caregility can make it easy to deploy intelligent devices and services to enhance patient care through virtual programs.”
Caregility Cloud™ allows health systems to easily centralize and scale programs such as Virtual Nursing, Virtual Patient Observation, Virtual Rounding, and Virtual Consultations in inpatient settings, improving staffing flexibility and workflow efficiency and making it easier to engage remote specialists and interpreters to support patient access and health equity. Trusted by more than 1,000 U.S. hospitals for high reliability, the platform is favored for its adaptability to a multitude of workflows and integrations with clinical platforms, including Epic.
About Baptist Health For more than a century, Baptist Health has delivered all its best in health care through Christian compassion and innovative services. Baptist Health, Arkansas’s most comprehensive healthcare organization, is here For You. For Life. – with more than 250 points of access that include twelve hospitals, urgent care centers, a senior living community, over 100 primary and specialty care clinics, a college with studies in nursing and allied health, and a graduate residency program. It is also the largest private not-for-profit healthcare organization based in Arkansas, providing care through the support of approximately 11,000 employees, groundbreaking treatments, renowned physicians and community outreach programs. For more information about Baptist Health, visit Baptist-Health.com, call Baptist Health HealthLine at 1-888-BAPTIST or download the myBaptistHealth app.
About Caregility Caregility (caregility.com) is a telehealth solution provider connecting care everywhere. Designated as the Best in KLAS® Virtual Care Platform (non-EMR) in 2021, 2022, and 2023, Caregility Cloud™ brings bedside care, virtual encounters, and AI capabilities together at the point of care. Doctors, nurses, and patients around the world rely on our intelligent telehealth edge devices and virtual nursing, observation, and engagement applications to enhance clinical insights, patient safety, and efficiency. Trusted by over 75 health systems, deployed in more than 1,000 hospitals, and supporting over 30,000 connected devices and millions of virtual sessions annually, Caregility is helping transform healthcare delivery across inpatient, outpatient, and home settings.
Tele-Neurology: Trends in Stroke Management and Brain Health
Virtual care is changing how stroke patients and those with complex brain and nervous system disorders are being treated and managed. This blog examines the adoption of tele-stroke programs and other tele-neurology use cases that are helping healthcare providers improve patient access and outcomes.
The important role that telemedicine plays in supporting acute care intervention through programs like tele-stroke is well documented. The research is clear: “Alerting neurologists via telemedicine that a patient with suspected acute stroke is en route to the hospital significantly enhances the speed at which thrombolysis is administered and increases the number of patients who receive timelier, potentially lifesaving treatment.”
Case in Point: In research exploring the impact of tele-neurology pre-notification during stroke cases, 50.4% of patients whose care team received a tele-neurology pre-notification received treatment within 30 minutes of arrival versus 18.9% of patients in the no pre-notification group.
High-acuity patient threats such as strokes demand rapid response and intervention to prevent severe brain damage and disability. Here are just a few examples of the ways leading healthcare organizations are improving patient care through tele-stroke programs:
Mayo Clinic has expanded its TeleStroke Network services across multiple states, ensuring that stroke expertise is just a video call away. The program has dramatically increased the timely use of thrombolytic therapies in rural hospitals. Learn more about Mayo Clinic’s tele-stroke network services.
Bringing tele-stroke into their digital-first approach, Kaiser Permanente’s integrated tele-stroke service offers immediate stroke assessments, reducing the time to treatment. Their model showcases a significant reduction in door-to-needle times and improved patient outcomes. Discover more about Kaiser Permanente’s integrated tele-stroke approach.
Cleveland Clinic developed a robust statewide tele-stroke network that serves patients across Ohio, ensuring rapid diagnosis and treatment. The network has been crucial in streamlining stroke care protocols and enhancing the accessibility of specialist consultations. Read more about Cleveland Clinic’s tele-stroke network.
Increasingly, providers are amplifying efforts around tele-neurology to extend the benefits of the virtual care model to patients who are recovering from strokes or other traumatic brain injuries. These patients often require closer monitoring and more frequent interventions due to memory impairment.
Telehealth programs like Virtual Patient Observation support around-the-clock care for these high-acuity patient populations, helping to reinforce patient safety and support. Virtual visits are also ideal for fielding follow-up care visits and symptom management for many neurological conditions.
And the field is ripe for further innovation. The incorporation of technologies like eye-tracking and computer vision into virtual care will unlock new possibilities in the field of remote clinical diagnostics for neurodegenerative conditions such as Alzheimer’s, autism, and Parkinson’s, where problems in the brain can often be detected in eye function.
The evolution of virtual care in neurology marks a pivotal shift in how strokes, brain injuries, and neurological disorders are treated and managed. Advances in technology have enabled widespread adoption of tele-stroke services, making specialist care immediately accessible, even in remote locations. As we continue to innovate, the potential to further decrease response times and improve outcomes through tele-neurology looks increasingly promising.
Healing Heros: Conversations About Veterans’ Healthcare Solutions and Telehealth
In the expansive realm of healthcare, Veterans grapple with a unique set of challenges that necessitate specialized attention. These challenges often stem from many factors, including the aftermath of military service, physical and mental health issues, and the complexities of transitioning back into civilian life.
Many Veterans find themselves facing additional hurdles in accessing the care they urgently require. This impacts not only the individual Veterans but also their families and the broader community, as delayed healthcare could contribute to the worsening of existing conditions and, in some cases, escalate into crises.
David Shulkin, MD
Enter Dr. David Shulkin, the Ninth Secretary of the U.S. Department of Veterans Affairs, whose leadership style proved instrumental in addressing the complex problems afflicting Veterans’ healthcare. Dr. Shulkin, recognizing the urgent need for change, set a visionary goal: to achieve same-day appointments for Veterans nationwide. This audacious objective was not merely an incremental adjustment but a transformative vision that aimed to overhaul the existing healthcare system for Veterans.
As a new member of Caregility’s Board of Directors, Dr. Shulkin endeavors to leverage his expertise to advance the company’s mission of pioneering innovative methods for remote healthcare delivery.
His visionary leadership has left an indelible mark on the landscape of Veterans’ healthcare, and in this interview, we unravel the complexities and unveil the exceptional solutions he implemented.
Dr. Shulkin, can you share your approach to leadership and how you fostered a positive organizational culture during your tenure as Secretary?
In my career, I’ve found that it’s easier to create bigger change than to do change through small increments. One of the issues when leaders try to make small changes is they get frustrated at how challenging it is to change the culture.
Being able to clearly articulate where you want your organization to go, why you want to create this change, how it’s going to be accomplished, a timeline, and an accountability plan are all crucial to effect change. Make sure your organization understands all those factors, that you’re consistent in your messaging, and that you put the resources within the organization behind that change initiative. As Secretary, I ensured our initiatives were Veteran-centric and tapped into the strong commitment to mission within the workforce to foster positive culture and change.
What strategies did you employ to improve the efficiency and effectiveness of the U.S. Department of Veterans Affairs?
When I entered the Department of Veterans Affairs, we had a situation where Veterans were waiting long periods of time for appointments. The clarity I brought was making it our priority to get those wait times down. I was clear that we’d set same-day appointments before the end of that year and the specific ways we’d do that were listed; using telehealth technology was one way, and allowing VA professionals to go across state lines was also part of that. We also gave advanced practice nurses independent practice authority, creating additional staffing opportunities to do that.
Efforts to make everyone accountable for that goal included actually publishing wait times publicly. Everyone could see what our goals were and whether we were achieving them. By the end of 2016, we had same-day appointments across the entire country at every VA facility. I believe we were able to accomplish that great change because there was clarity around what our objective was.
How did you navigate budgetary challenges and allocate resources to ensure Veterans received the necessary care and support?
The easiest answer when things are not performing the way anyone wants is, “Well, we don’t have enough money,” and I don’t think that is usually the answer. There are times that is true, but in my experience with the VA that was not the case. Congress would always allocate the money we needed to care for Veterans. The harder part is designing systems meant to get the results you want that are optimally performing, like finding ways to get your workforce to operate at their highest level of training or licensure and letting others field lower-level tasks or using technology to increase labor productivity but decrease the time to perform tasks to look for new, more cost-efficient ways to practice. That’s hard to do but it ultimately saves money if implemented well.
As a new member of Caregility’s Board of Directors, what specific goals do you have in mind for the company’s role in pioneering innovative methods to deliver healthcare remotely?
Healthcare has been one of the few industries in our economy that has not seen labor productivity improvements over the past decade. Instead, we continue to struggle with labor shortages and increasing costs. For a health system to get real value from technology it must be versatile and integrate into the current workflow. Caregility seeks to be the enterprise solution for health systems that seek to use technology to improve efficiency and outcomes.
Looking ahead, what emerging trends or technologies do you foresee playing a significant role in shaping the future of telehealth, and how can Caregility position itself to stay at the forefront of these developments?
Future strides in telehealth are going to be dependent upon the ability to integrate data sources, personalize care options, integrate care delivery among various disciplines, and use artificial intelligence and large language models to extract information from clinical and administrative data to better inform diagnosis and treatment options for patients.
Homelessness among Veterans is a persistent issue. What strategies did you employ to address and reduce homelessness within the veteran population?
We awarded grants to groups that operated in the communities. We also worked closely with HUD to expand the use of HUD-VASH vouchers for housing, including expanding benefits to Veterans beyond those who were honorably discharged.
How did you ensure and measure the quality of healthcare provided to Veterans within the VA system?
We measured quality using and comparing quality metrics in the private sector. We then published all our quality measures. When you look at the VA’s publicly reported outcomes compared to the private sector, the VA overall outperforms the private sector. This surprises many people. It demonstrates that an integrated system of care that can follow patients longitudinally and has a system based largely in primary care with strong integration with behavioral health does have better outcomes.
That doesn’t mean the VA is best at everything. At the system level, it’s superior because private organizations often experience gaps in care. Care should still be an individual choice though. Sometimes you can get the best care for you within the community you live in. Or perhaps you need a heart transplant, and the best provider is a non-VA facility. You may need a treatment that the private hospital does better than the VA. You want to have a system of care that is transparent enough that you can actually look and see, “Is that the best care for me? Is it VA or a private system?” We need to be educated enough as consumers to make that call.
During your tenure, the VA faced various challenges. Can you discuss a specific crisis or challenging situation and how you managed it effectively?
The wait time crisis was our biggest challenge at the VA. We ultimately achieved same-day appointments for all urgent Veteran healthcare.
There is a lot to be learned from the VA in terms of the integrated system of care, chronic care management, behavioral health integration, incorporating the social determinants of health into care planning, and decreasing access barriers like high copays and deductibles.
Transparency is good for healthcare and it’s good for patients. If we can provide that information in an accurate way, we can improve the whole health system. That was my goal at the VA. Wherever you can shine light on issues, people will make better decisions.
Rural Veterans often face unique challenges in accessing healthcare. What initiatives did you undertake to address healthcare disparities in rural areas?
We had an office of rural health that addressed issues with home-based care, remote monitoring, and telehealth.
Women Veterans have distinct healthcare needs. What steps were taken to ensure that the VA adequately addressed the healthcare and support requirements of women veterans?
We created women’s health clinics in each of our medical centers and initiated new programs and policies and increased funding.
Given the advancements in technology, how did you integrate telehealth services to improve accessibility for Veterans, especially those in remote or underserved areas?
Tech needs to be a big part of a solution in accessing care where you don’t have physical facilities or the workforce distribution. There are other ways of addressing the access issue besides pure tech, but I primarily think that should be the essence of the solution – get people to care wherever the expertise exists.
Other solutions include things like working with educational programs to do workforce training and to promote greater patient and family caregiver training to help people understand how they can be part of improving health in their communities, implementing preventative strategies, using tools like AI to help people get information on when they should access specialty care versus primary care versus urgent care, and the expansion of telehealth and remote monitoring care in the patient home and community. People want care where it’s most convenient for them. To me, that means either care on your phone where it’s mobile or care in your home.
Looking back on your tenure, what do you consider to be your most significant accomplishments, and what lessons did you learn that could benefit future leaders of the Department of Veterans Affairs [or health systems in general]?
Creating a system of integrated VA and community-based care that served the Veteran is what I perceive to be our most significant accomplishment.
My advice for others is that incremental change is overrated. Sometimes big goals, while risky, are the way to achieve great things. It’s important for every organization to ask, “What’s a goal that would make a big difference that would be wise for us to pursue?”
Healthcare organizations have the responsibility to answer that question for their specific communities. Healthcare is geographic. Look at what clinical priorities there are for different patient populations in your community. Certain populations have a higher incidence of diabetes, for example. Look at not only the problems but how you’re trying to solve them. Be more proactive in outreach to solve problems.
Many healthcare organizations still have a model where they wait until a patient has a problem and then schedule an appointment to bring them in. Organizations need to think about how we can reach out to people in the community to intervene and manage conditions better or prevent them from having to come to the hospital.
In the Department of Veterans Affairs, when I became aware of drugs that can cure Hepatitis C, we looked at how many Veterans had Hepatitis. There were 176,000 patients documented in our database. We reached out to all of them to bring them in for the treatments that can cure that disease. By doing so, we were able to get it to less than 10,000 untreated Veterans. That proactive outreach model of intervention is extremely powerful.
Read the Impaakt article where this interview was originally published here.
Hybrid Care Innovation at UMass Memorial Health
Digital innovation is a cornerstone of UMass Memorial Health’s strategy, garnering the health system impressive accolades including HIMSS Stage 7 certification for EMR adoption, CHIME’s Most Wired Level 8 certification, and Epic Gold Stars Level 10 status.
Dave Smith, Senior Director of Digital Innovation for UMass Memorial Health, attributes his organization’s competitive edge to a physician-led leadership team that truly embraces digital transformation. UMass Memorial has been delivering hybrid care for the better part of 20 years through its flagship eICU and tele-stroke programs. The throes of the pandemic and ensuing challenges related to patient safety, capacity management, patient flow, and staffing shortages reignited interest in hybrid care innovation, leading the health system to pursue additional programs like hospital at home, remote observation, and remote patient monitoring (RPM) in recent years.
In the enlightening session “Hybrid Care Innovation: The ROI of Bedside Virtual Care at Scale,” part of Becker’s Healthcare’s 2024 Digital Health and Telehealth Virtual Event, Smith sat down with Caregility President and COO Mike Brandofino to share compelling insights into the transformative hybrid care initiatives his organization is pursuing, how his team approaches ROI, and what it takes to scale new hybrid care models.
Hybrid Care’s Return on Value
UMass Memorial’s Hospital-at-Home program is a great example of how health systems are bringing resources to bear to improve outcomes, efficiency, and the experience for patients and clinicians. Patients receive twice-daily visits at home, supported by EMS partners working in collaboration with UMass doctors and nurses. They also have immediate access to virtual nursing support. The health system employs a four-to-one ratio for field nurses and a 30-to-one ratio for virtual nurses.
By bringing acute care to the patient’s home, the team has been able to expand capacity. “In our first year of operation, we saved over 3,000 bed days at our busiest hospitals,” shared Smith.
“With our eICU program, we monitor 150 critical care beds around the clock with intensivists on any given shift and the aid of a pharmacist at night,” Smith said. Since its inception in 2006, UMass’s eICU program has seen a 27% reduction in patient mortality and fewer patient complications, reducing care costs.
“For programs like tele-stroke and tele-psych, the ROI is really about improving access,” Smith continued. “But also, community hospitals see the ROI because they don’t have to hire and retain a full-time specialist. Instead, they buy professional services from a tertiary health system like UMass Memorial.”
The health system’s remote video monitoring (RVM) program has shown the strongest direct labor-cost ROI by enabling a single care team member to support six patients instead of conventional one-on-one observation ratios. “To take advantage of the full 12-patient panel, we assign each observation tech six primary patients and six backup patients for a total of 12,” Smith shared. “For every remote observation tech, we save $300,000 a year in direct labor costs.”
The health system is also leveraging AI solutions for radiology, ophthalmology, and ambient dictation to save providers valuable time. “I don’t think AI is going to replace doctors anytime soon, but I do think the ones who embrace it will probably surpass the ones who don’t,” noted Smith.
Scaling Hybrid Care Innovation
Smith sees digital health innovation as “the cost of doing business for healthcare systems that want to innovate and remain competitive.”
“We're in the process of building a new 72-bed inpatient facility that will open about a year from now and every bed will be wired with Caregility technology. We'll use the technology for a variety of use cases like virtual rounding, remote observation, specialty consults, patient/family communication, and even tele-ICU level care. And the funny thing is, it was an easy sell to hospital leadership because they understand the importance of hybrid care and balancing staffing demands. I just think hybrid care is the new standard.”
Dave Smith
Senior Director of Digital Innovation, UMass Memorial Health
Smith champions platforms that can be leveraged across the enterprise over point solutions. “To do anything at scale, it cannot exist in silos and pockets that are scattered throughout the organization,” he shared. “A good example is our commitment to building a digital medicine hub. We’re taking most of our virtual services and putting them under one roof. By doing so, not only will it be a showcase for our health system of the future, but we’re expecting to find operational synergies by having these virtual care teams collaborate in the same physical space. So, teams like eICU, transfer center, RVM, RPM, interpreter services, and virtual nursing will all be working alongside each other.”
“We’re also investing in a new digital innovation team to support rapid scalability. Digital health and especially AI is evolving so quickly that we need to operate at a faster pace to keep up. I’ll be leading a new multidisciplinary team to focus on emerging technologies that support our system initiatives and foster collaboration with our care teams. The whole idea is to identify opportunities, experiment with proofs of concept, fail fast, if necessary, iterate, and then deliver a solution or look at alternatives.”
“People are embracing technology in ways never thought possible and it’s making hybrid care models not only plausible but also practical.”