Virtual Care ROI with Dan D’Orazio of Sage Growth Partners
Digital Health Frontiers – Podcast Ep. 5
Dan D’Orazio CEO, Sage Growth Partners
Mike Brandofino President and COO, Caregility
In this episode of the Digital Health Frontiers podcast, host and Caregility President and COO Mike Brandofino is joined by Dan D’Orazio, CEO of Sage Growth Partners, and Caregility CFO Tod Nestor for a candid conversation about virtual care ROI. Mike, Dan, and Tod dig into market research findings and executive feedback on what’s driving health systems to go all in on telehealth, from the hospital bedside to the patient’s home.
Dan contrasts healthcare spending from 2000 to 2024, emphasizing the dramatic growth in hospital costs and the rising demand for more efficient care models. He attributes the push for virtual care to a “perfect storm” of factors, including an aging population, sicker patients, labor shortages, and rising healthcare expenses. Tod offers insights into how CFOs evaluate the ROI of virtual care investments, noting their growing demand for evidence-based, measurable savings. The conversation highlights real-world examples of successful virtual care implementations by healthcare organizations that embraced virtual care to modernize workflows and improve care delivery despite limited funding.
Listen in or read the full transcript below!
Read the Transcript
Welcome to Digital Health Frontiers, where we explore the cutting edge of healthcare technology, policy, and innovation, hosted by Mike Brandofino, President and COO of Caregility. In this episode, Mike is joined by Dan D’Orazio, CEO of Sage Growth Partners, and Caregility CFO Tod Nestor for a candid conversation about virtual care ROI. Mike, Dan, and Tod dig into market research findings and executive feedback on what’s driving health systems to go all in on telehealth, from the hospital bedside to the patient’s home.
Mike Brandofino Hey everybody. Welcome to Caregility’s podcast. I’m Mike Brandofino, President and COO of Caregility, and I’d like to introduce Dan D’Orazio from Sage, a company that we’ve been working with to do an economic value calculator, and Tod Nestor, our CFO here at Caregility. Dan, you know, what we’ve been working on has really been trying to identify the key drivers that really help customers figure out that economic value in virtual care systems. We’re seeing customers expand or looking to expand virtual care to every room and we really are trying to nail down for them some of those key drivers. Can you talk about that?
Dan D’Orazio Yeah. Thank you for having me, Tod and Mike. Great to work with the Caregility team. I think it’s interesting if we look back 24 years to look forward 24 years. And here’s what I mean. In 2000, we spent $1.4 trillion on the entire U.S. healthcare economy. In 2024, we spent 1.4 trillion just on the hospital, part A alone.
And so, Mike, you’re asking about, you know, why are people looking to expand to virtual care? The growth of our hospital-centric model is enormous. We have more and more people aging in, and they’re becoming sicker and sicker, and we have eventually fewer and less experienced staff. So, you put those factors together and you say, well, how am I going to deliver care effectively and efficiently across space and time? And I even mean inside the walls of an organization, not even outside the walls of an organization. We’re considering both of those in these conversations. And so you look at the shortage of supply capacity expertise, you put on top of that labor expense, the challenges that exist generally in healthcare with sharing information easily, you know, across many different domains in many different settings – I think you have an unfortunate perfect storm that brings us to this conversation of how do we solve this problem, which has given rise to the virtual care discussion.
Mike Brandofino Yeah, I definitely think that from a staffing perspective, you know, that’s a clear issue. I think everybody understands that. I think the challenges as we get into talking with customers are, you know, where is the CFO’s head on all this? And, you know, how do we get them to understand current and future economic value benefits?
Dan D’Orazio Yes. Yeah, I agree. And Sage and the work we’ve done with you, we build what we call economic impact models because we’re trying to understand a couple of things. What is the use case of the problem we’re solving? What is the workflow? And where do we generate revenue, reduce cost, or save time, generally speaking? And when we are talking about time, it’s not necessarily getting rid of people. We already have a shortage. It’s how do we spend more time doing more of what we could, should, and need to across the different skill sets? And, Tod, you being the CFO – we often sort of tongue-in-cheek call the CFO the CF-“No” because they have a lot of people knocking on their door telling them that there’s going to be great ROI, which is important but often elusive to chase and maybe even arbitrate – but how have you been unpacking this model and what have those conversations been like with your colleagues on the system side?
Tod Nestor Dan, thanks for asking. I think one of the things that we’re seeing is the CFOs are re-entering some of the decision-making on the resource allocations. Maybe during COVID they were less so because the focus was on just providing care. As the CFOs re-enter some of the decision-making on the allocation of resources, I think the bar is going up on what they want to see. What’s required? I think when you talk about the savings opportunities, you know, CFOs by nature are going to want to be fact-based. Maybe that’s why that friendly term of CF-”No” occurs – they want to see some more support for the decision-making and the resource allocation.
And so what we’ve been seeing is, you know, their skepticism around that. There’s the challenge of change management within an organization. And what’s required with virtual care and telehealth? But ultimately what we’re seeing is a desire for more substance in making the decisions, not a lack of a desire to do it, but more support for making that decision to allocate the resources to an effort like this. That’s all they’re looking for and the calculator and some of the what I’ll call hard savings that we can identify through the drivers of cost savings as well. Some of the cost savings are going a long way to conquering some of those challenges of the skepticism that we’re seeing from the CFO ranks. We also are seeing it’s not only about that though. There is a strong desire for all executives and hospital systems for improving healthcare just as much as there is about the savings. So, they’re wanting to see both of those results.
Dan D’Orazio Yeah, very helpful. Mike, I was curious – in your conversations, are these light-switch-moments for people wanting to see, you know, like we talked about, ROI, but is this like ‘Hey Mike, you said you’re going to offer me the solution tomorrow. What do I see?’
Mike Brandofino Yeah, in some cases it is. But I think, you know, Tod getting involved and talking to CFOs is a really good step for some of our customers. I think that the challenge is we focus heavily on the clinical side, which is clearly right when helping them develop workflows and improve care, or modernize care, but they’re not always well-versed in making the pitch. One of the things that we’re trying to do is help educate the clinical side and then, on the CFO side, is the idea of these building blocks. You can’t get to the Holy Grail of ROI in health systems – which is most likely improved ratios, you know, improved caregiver-to-patient ratios – until you buy back some of the time. Until you buy back enough time for nurses to practice at the top of their license, you can’t get to those.
So really what we’re trying to educate customers on is the building blocks of getting to the bigger hard-dollar ROI. And that could be in the form of, you know, improving discharges by 40 minutes or 30 minutes and improving patient satisfaction scores, which, by the way, enables caregivers to use virtual care nurses a little bit more than floor nurses potentially, too. It maybe takes some of the workload off of mundane tasks that nurses have to do every day that you might be able to push to lower-skill people. Then keep, like I said, buying that time back to the point where, before you know it, you don’t have to tell nurses that you’re increasing your ratios. They will by the sheer fact that they have the extra time. So I think those building blocks are really important to talk to our customers about and also educate and help our clinical-side partners and stakeholders build the pitch, if you will, based on those building blocks.
Dan D’Orazio Yeah, that’s a great point.
Mike Brandofino So, you know, when you’re out there, Dan, you know there are obviously key areas of value that consistently pop up. What are the top two or three that pop up all the time?
Dan D’Orazio Yeah, so, I think resources and time, and of course, they’re connected. And let me unpack those a little further. Nurses do an average of 72 tasks an hour, an average of 55 seconds per task, and I’ve seen this through the research. I also have a wife who’s a clinical care and trauma nurse who’s also a nurse manager and you just see what they wrestle with, you know, inside the walls of the hospital when you’re looking at that volume of tasks that they have to perform. You talk about how the ratios will come when we give them the time to do what they’re good at and trained to do, and think, and be the glue that keeps the operations running literally and figuratively. In an organization that’s providing care, resources are not just about nurses, but also all the other ancillary support providers. And that time is so valuable. But it’s hard to exactly put your finger on until you give it back to someone, right? So if you go from 55 tasks an hour to 40 – and you talked about patient satisfaction, Mike – the studies are clear: Happy nurse, happy patient. And that relationship is causal and direct. And that’s where we have to get connected.
And then sort of, this deferring of clinical cost because if we’re getting to stuff sooner, if we’re doing the proper interventions, if we’re thinking, we can also get people out, to your point, from a discharge perspective sooner. Now we know the last day of that discharge is the cheapest, but the person coming into that bed, that first day is not the cheapest for them, right? And so, that’s where all these resources go, you know. It’s one flip from out-the-door to in-the-door and so that’s where time and resources in that clinical movement or deferring of cost really becomes important. And this is what people are looking for in these conversations.
And I would proffer that of all the years we’ve built these models, no one expects a vendor to have all the data. The clients don’t even have it. It’s ‘how do we partner on this to really figure out what’s going to work for our unique system of care, in our unique problems?’ And that’s the partnership that they’re looking for. And so Mike, this is exciting. But let’s talk about a little bit of what you’re seeing with your clients, right? How do we bring this into reality and bring this to life a little bit? Could you give a couple examples of where this is happening in the partnerships that you have and what are or what kind of results are people seeing, albeit different, I’m sure?
Mike Brandofino Sure, yeah. We have a couple of great examples. And it’s interesting, you know, as we talk about economic value, you, I think, immediately start thinking this must be reserved for health systems that have a ton of money and ability to invest and actually we’re seeing adoption across the board.
So I’ll give you an example. One of our customers, Baptist Health Little Rock, they’re in a state that has the least funding of all 50 states from the federal government. Yet the leadership of Baptist understood that in order for them to be able to deliver the care, modernize care, and work the resources they had, they had to commit to putting virtual care in every room. So, they found a way. And in their model, they’ve committed to putting virtual care in every room. I think there, over 50-60% of the rooms are ready and the feedback that they’re getting from the staff has been incredible. In fact, you know, health systems or hospitals that they haven’t gotten to yet and floors they haven’t gotten to yet are like, ‘When are we getting our technology?’ They’re really seeing the benefit of it. And from their perspective, they, you know, kind of put the cart before the horse. They said we understand we need to do this. We know we’ll get the benefit, the economic benefits. But we can’t wait until proving all of that. And so, they went ahead and they did it, you know, on basically the idea that they need to modernize care.
Another one down South, Lee Health, is another customer who in fact went through it. They just recently went from public to private, so they also were losing a bunch of federal funding. But the leadership didn’t bat an eyelash. They’re on the path of this commitment to putting virtual care in every room. They’re building that and they believe in that building block approach, by the way. You know Doctor Carracino, the CMIO over there, and I have had many conversations about, you know, just getting the little wins, adding workflows, adding more capability. And before you know it, you start seeing those building blocks lead to, you know, significant real dollar value.
Here are two great examples of health systems that aren’t the biggest, you know, in the country. They’re pretty big in their region, but they made those decisions in advance of a full hard dollar ROI because they just saw the value. And I think that’s really something that we need to figure out how to help more of our customers do, you know? Tod, as you talk to CEOs and you hear the skepticism from them, do you think these types of stories can help and move them along? I think you either mentioned it or I definitely know you have talked about it before – we’re seeing customers talk about this as an investment in the future. What have those conversations been like? What are your thoughts?
Tod Nestor Great question. I want to build a little bit on what you and Dan both have said. At the end of the day, what I’m hearing from CFOs and CEOs, as well, is their challenge is they have limited people resources and monetary resources. So, they need to figure out where to put it to its best use, and it is those investment opportunities you’re talking about. So, as we develop approaches to help them identify where they can either have that hard-cost savings or even soft-cost savings, which allows them to reallocate it to other applications or a nurse’s time. As Dan said, they can improve the quality of care, they can see better outcomes, they can have other intangible benefits that occur that are eventually tangible, and you can quantify. So having that ability to talk to them in terms of resource allocation – where they invest those freed-up resources as a result of the virtual care in every room – is something that’s happening and it’s resonating. You see their heads nod when we talk about it.
I think one of the things that you know we’re doing to help with some of that skepticism is we’re developing approaches to allow them to actually measure and monitor that after they put it in place as well. So they can measure those savings and those resources as a way of doing business going forward. That helps them with that resource allocation because at the end of the day, the CFO’s role is not so much about saying no, it’s about saying, you know, where can we get our best return on our investment? And that is maybe in the quality of care or in some kind of cost savings. It doesn’t always flow to the bottom line in a hospital system. Sometimes it’s about putting those resources to better usage and improving the quality of care just as well.
Mike Brandofino Thanks, Tod. So Dan, you know, as we wrap up here – one of the things that we’re also seeing and believe strongly in is that virtual care and the modernization of care is going to apply outside of the four walls of a hospital. And you mentioned it a little bit before – the ageing population. So, long term care, home health, and aging-at-home are definitely going to benefit from virtual care. I guess the question is looking ahead. How do we create the economic value there and where do you see it heading in the next, you know, three to five years?
Dan D’Orazio A report last week highlighted the funding boom and investment in ambulatory property and sites of care in the US. I think that’s for a couple of reasons but is primarily driven by the fact that people want to be there more. Also, we know, again, that 1.4 trillion is everything we spend just on hospital now. And it used to be everything 20 years ago, 24 years ago. So, the price and resource consumption are not viable. So, both from a consumer patient perspective and Medicare, who is, you know, for over 65, the largest payer – they have a need to, I don’t want to say rationalize, but be rational about the cost of care. And we know if anything, healthcare is difficult operationally, right, because there are so many different crevices and cracks and maneuvers that people have to make. And when you can bring your team together virtually, it’s hard to do that within a hospital, right? And so, when someone leaves, the last thing you want is someone going from a hospital to a skilled nursing facility to come back to the hospital. There are virtual hospitalists, you’re seeing all kinds of virtual psychiatry, and virtual specialists that can go, you know, to the 30 or 40 million people in rural America who actually can’t get to any kind of care that’s close.
But this is not just about folks that are far away. I see a need for this inside the walls and then outside the walls right to that person’s home. That might be five miles away in that catchment area. We have to smooth out the experience and this is the most important thing for the provider and the patient. We cannot have a disjointed experience, for one, and a good experience for the other because it will fail. And during COVID, what we saw was everyone stopped. All the challenges went away. Providers and patients felt the benefit. We have to continue to move and, you know, I think that’s where you guys are focusing. How do both ends of this equation work? Because, if not, it won’t work.
Mike Brandofino Yeah, I agree. You know, I think the consumerization of care is something that we should all be thinking about and I think that speaks to what you said about the experience. Think about 15, 20 years ago how we used to plan travel through a travel agent. Now we all do it on our phone. I think people want the same thing with their healthcare, and I think we’ve made strides. COVID forced us to, but I think we need to continue to drive down that path. And I think this whole modernization of care, having the ability to have virtual everywhere, will really enable that and make it easier to provide. But there’s a lot of challenges in there in between.
Well, guys, thank you very much for the conversation. Hopefully people who are listening. If you’re interested in hearing more about the economic value calculator, please reach out to us at caregility.com. And, again, thank you for joining, Dan, and thanks for joining, Tod.
Dan D’Orazio Yeah, my pleasure. Thanks for having us.
Summary: Bridging IT & Clinical for Virtual Nursing Success
The on-demand webinar “Bridging IT and Clinical Worlds for Virtual Nursing Success,” hosted by the College of Healthcare Information Management Executives (CHIME), features insights from Lee Health’s System Director of Virtual Health and Telemedicine, Jon Witenko, Business Analyst Kimberly Gualt, and Caregility’s President and COO, Mike Brandofino. They discuss their experience implementing and scaling virtual nursing and the collaborative strategies necessary to ensure success.
Key Themes and Takeaways:
1. Cultivating Clinical and IT Alignment
Successful virtual nursing programs hinge on strong collaboration between IT and clinical teams.
The speakers stress the importance of mutual understanding, where IT appreciates the nuances of clinical workflows, and clinicians understand the technological capabilities and constraints.
2. Addressing Implementation Challenges
Common hurdles include resistance to change, technical barriers, and scalability concerns.
The session highlights lessons learned from overcoming these barriers, emphasizing the importance of phased rollouts and continuous feedback loops.
3. Seamless Clinical Workflow Integration
Integration is key to preventing disruption in day-to-day care delivery.
The discussion underscores designing solutions that complement, rather than complicate, existing workflows, ensuring minimal disruption to bedside care.
4. Virtual Nurse Training Strategies
Preparing nurses to adopt virtual care roles is essential.
Lee Health shares strategies for equipping virtual nurses with the skills to engage patients effectively through technology while maintaining empathy and clinical excellence.
5. Patient Impact
The program demonstrates measurable benefits for patients, including enhanced monitoring, reduced response times, and improved access to care.
The panelists emphasize maintaining the human touch even in a technology-driven model to improve patient satisfaction and outcomes.
6. Staff Reception
Ensuring team-wide support is a critical component of success.
The discussion touches on addressing skepticism, demonstrating the value of virtual nursing, and involving staff early in the process.
7. Evolving Role of Virtual Nursing
Virtual nursing is a scalable, cost-effective solution to address workforce shortages and rising patient acuity.
The conversation speculates on how the role might evolve with advancements in AI and telehealth technology, moving toward more proactive and preventive care models.
Insights for Healthcare Professionals
The on-demand webinar provides actionable insights, including:
Creating alignment frameworks to bring IT and clinical teams together.
Adopting an iterative approach to tech deployment, allowing for adjustments based on real-world use.
Leveraging metrics and data to measure success and identify areas for improvement.
This session ultimately highlights how fostering collaboration, planning for adaptability, and prioritizing patient and staff experiences are critical for achieving sustainable success in virtual nursing programs.
by Kedar Ganta, Chief Product and Engineering Officer, Caregility
This is my final post of the year, and I would like to take a moment to share some key highlights that reflect our commitment to innovation and continuous improvement.
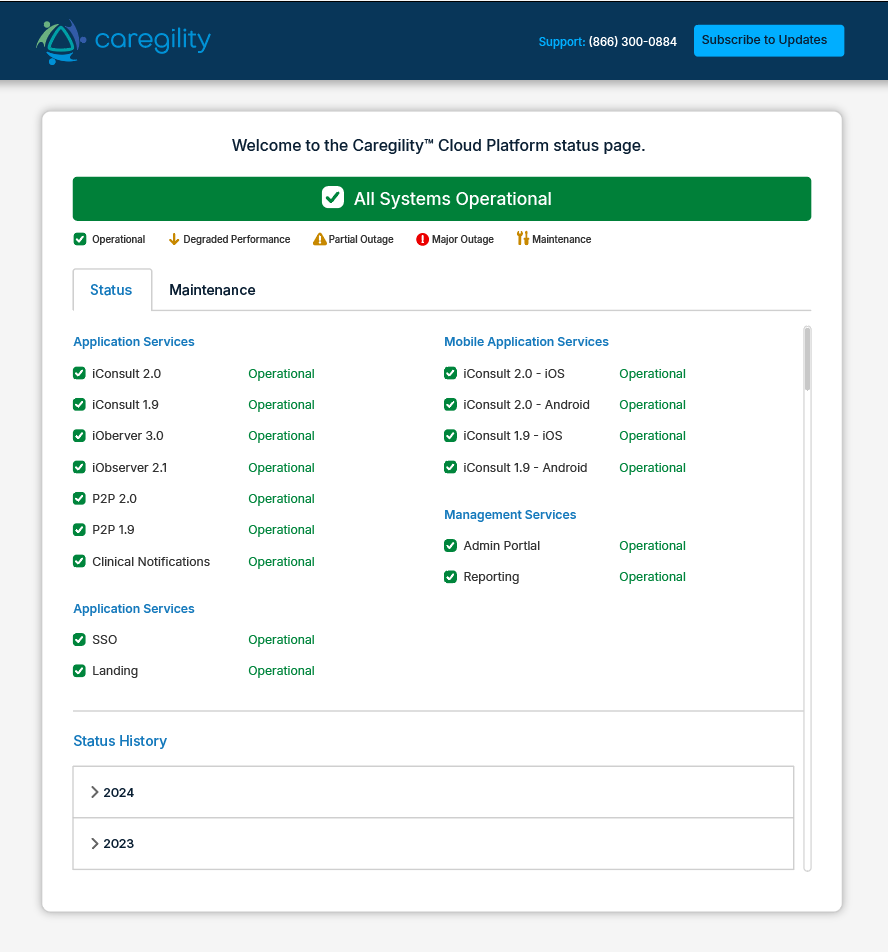
In 2024, we successfully rolled out 20 releases including 6 major updates and 14 minor ones. These releases were designed to improve your experience and keep us moving forward. We also launched a new status page (https://status.caregility.com) to provide real-time updates on the status of the Caregility applications to always keep you informed about our platform’s reliability.
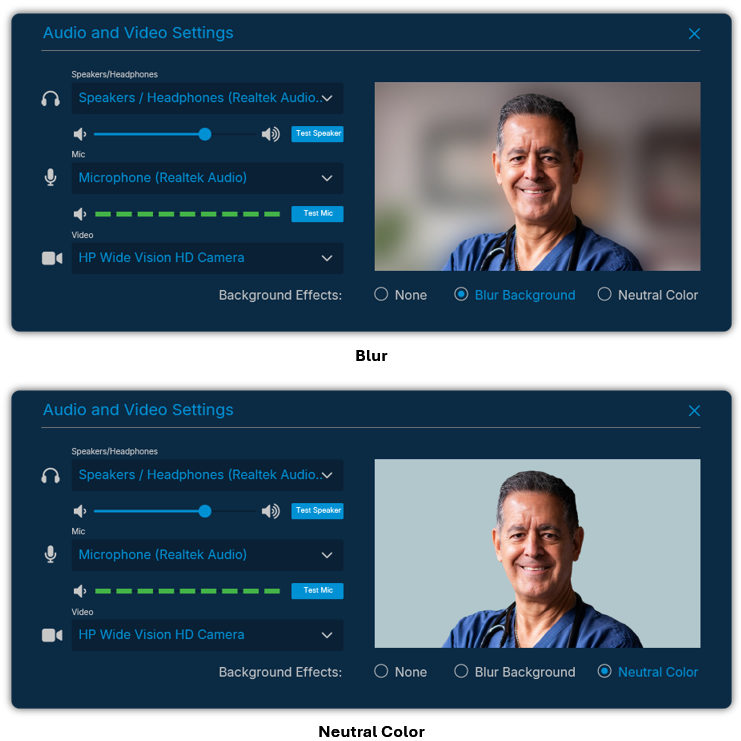
With the November 2024 release, we introduced a new virtual background feature in iConsult. This enhancement minimizes distractions by removing irrelevant background elements during virtual sessions. For now, you can blur or set a neutral color as your background, and in future releases, we will offer the ability to choose and personalize your background for a more tailored experience.
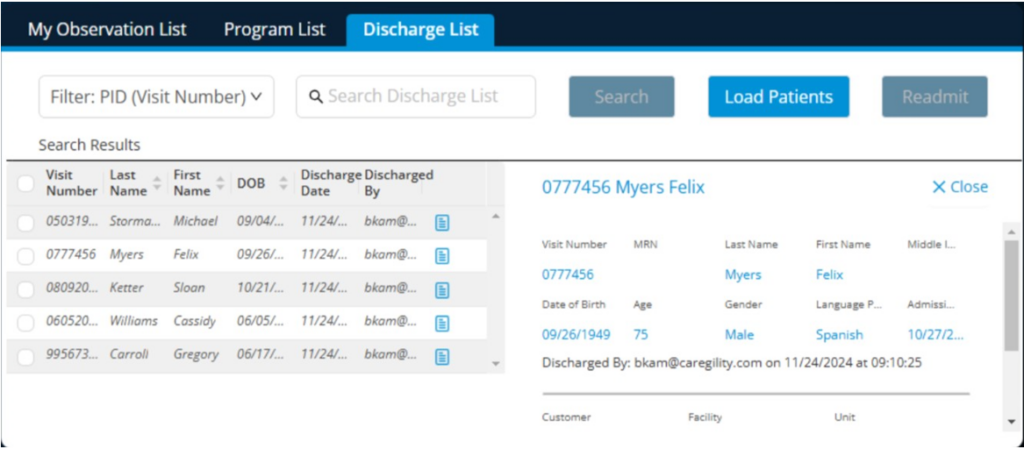
In iObserver, we made significant improvements to the way observers interact with live sessions. The recent release enables multi-camera streaming with independent 5x and 40x options on the APS 200 Duo and APS 100 Pro + Flex Cam endpoints, offering greater flexibility and detail. We also enhanced the Discharge List to provide increased visibility by tracking when and by whom patients are discharged. Color-coded tooltips and additional language phrases improve usability and accessibility.
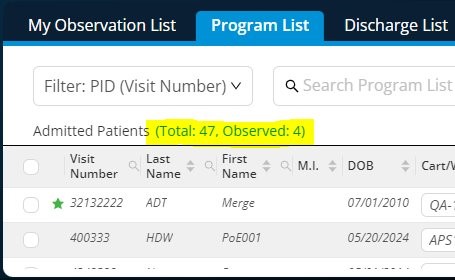
iObserver 3.0 also introduces Admitted Patient Statistics to the Program List, offering quick insights into patients on the list and those under observation. Look out for even more enhancements, including real-time reporting on active sessions, device availability, and assignment metrics in future updates.
Meanwhile, the Admin Portal is evolving into a central command hub, making device management more intuitive. With new features like scheduling soft reboots on APS endpoints, we aim to streamline operations and minimize downtime to better support your needs.
As 2024 draws to a close, I want to thank you for your feedback and engagement throughout the year. Wishing you all a happy holiday season, and I look forward to continuing our conversation in the new year!
When you picture the hospital of the future, it’s hard to imagine patient rooms without remote monitoring, virtual observation and some form of AI as core capabilities. As health systems face continued financial and workforce pressures, that invariably leads to the question of how to modernize care. The inevitable conclusion is that it must involve patient rooms that are always connected and patient-aware.
Fortunately, the integration of virtual care and AI at the bedside is fueling a transformative shift in healthcare delivery that will allow for these types of patient rooms. Audio, video and sensor-based technologies are unlocking additional clinical insights and engagement avenues for care teams, creating a foundation for innovation. Inpatient care programs like virtual nursing, virtual sitting and virtual rounding are already helping health systems offset challenges while delivering significant benefits for patients and staff.
The challenge lies in navigating the path from today’s reality to widescale implementation among competing priorities and project budgets. This degree of transformation doesn’t happen overnight. As healthcare executives build their roadmap for modernizing care, they want evidence of key value drivers in their IT investments, balancing the cost of scaling implementation against near- and long-term goals. Understanding the economic impact of care programs is crucial for strategic planning and resource allocation.
To better understand the critical areas where healthcare organizations see return on investment (ROI) in technology-assisted clinical workflow optimization, Caregility and Sage Growth Partners partnered to examine trends and determine what kind of tool could help health systems support the mass deployment of modern technology in every patient room.
Caregility and Sage conducted in-depth interviews with leading health systems across the U.S. to identify where healthcare organizations are realizing ROI from inpatient virtual care initiatives. Three key areas of impact and one fundamental truth were uncovered. The fundamental truth is that there’s no silver bullet that provides all the real-dollar ROI that most chief financial officers (CFOs) are looking for. However, there are essential initial steps and building blocks that come together to create a strong foundation of economic value that leads to a bigger financial ROI.
These building blocks buy back time for staff, enabling them to focus on tasks that are more impactful. This also enables organizations to increase ratios where appropriate, which leads to real-dollar ROI.
The three areas of impact are:
1. Resource cost reduction
One of the most compelling drivers of economic impact from virtual acute-care models is the ability to reduce staffing resource costs, particularly in nursing. Virtual nursing offloads a significant portion of the administrative burden that falls on bedside nurses. By shifting tasks like admissions and discharges to virtual nurses, organizations are freeing up bedside nurses to field higher-value tasks. This recouped time reduces costs associated with incidental overtime for bedside nurses.
With the tools to redistribute clinical tasks in place, hospitals can optimize their workforce to reduce reliance on costly temporary staffing or agency nurses. Nurses report improved job satisfaction due to the collaborative care approach, leading to reduced turnover and recruitment costs. With average turnover costs per nurse totaling roughly $56,280, reducing turnover by just 10% can bring significant savings.
Telehealth-enabled acute care also allows health systems to extend the reach of physician specialists to satellite locations instead of hiring dedicated staff at sites with low utilization. Virtual engagement reduces the “windshield time” lost during commutes between locations.
2. Clinical cost deferment
Another recurring area of financial impact validated during research is the ability of virtual acute-care programs to help prevent hospital-acquired conditions, which add substantial costs to inpatient care. Health systems reported reductions in catheter-associated urinary tract infections (CAUTI), central line-associated bloodstream infections (CLABSI), pressure injuries and patient falls. These improvements are attributed to enhanced monitoring capabilities and greater adherence to clinical best practices made possible by the focused support of virtual clinicians.
Preventing these conditions reduces costs, shortens hospital stays and improves patient satisfaction and throughput. Hospitals can also avoid readmissions and associated costs by using virtual bedside engagement to enhance the discharge processes and ensure patients leave the hospital with better education and support.
Although this research initiative looked at acute virtual care’s impact on intervention in patient falls, CAUTI, CLABSI and pressure injuries specifically, additional patient outcomes stand to benefit from similar targeted clinical quality improvement efforts.
3. Savings from recouped bedside hours
Time is one of the most valuable commodities in healthcare. Virtual acute-care initiatives offer hospitals a way to reclaim bedside hours. Virtual nursing task redistribution allows bedside nurses to focus on direct patient care, working at the top of their license rather than being bogged down by administrative duties.
Hospitals report saving up to 25% of the time bedside nurses typically spend on documentation by fielding admissions virtually. Virtual discharges save bedside nurses up to 67% of the time typically spent on discharge paperwork. For the average hospital, this cumulative time savings translates to the equivalent of multiple full-time nursing employees.
While the economic impacts are compelling, the benefits of inpatient telehealth programs extend far beyond the bottom line. These initiatives create a ripple effect of positive outcomes that touch every aspect of healthcare delivery. Executives observed virtual acute-care wins that are harder to quantify financially, including the ability to retain experienced nurses nearing retirement by redeploying them to virtual roles. In addition, they reported seeing a 20% spike in patient satisfaction reflected in HCAHPS scores due to the uninterrupted nature of virtual interaction, as well as overwhelming staff satisfaction with on-demand access to remote clinical support at the bedside.
There is common consensus on the broad applicability of video-based engagement and AI-assisted monitoring at every bedside. The downstream effects on patient capacity and throughput and the implications for revised ratios built with cross-collaborative care teams in mind make a compelling case for continued expansion. The experience gained from inpatient virtual care programs also lays crucial groundwork for expanding into home-based care models.
These future-facing technologies are key to modernizing healthcare delivery and creating more proactive, continuous care models. It’s not just about meeting current operational demands – it’s about elevating what’s possible in healthcare. As care continues to evolve, organizations that have embraced virtual engagement and AI at the bedside will have the infrastructure and experience necessary to seamlessly incorporate new technologies and care models, ensuring they remain at the forefront of healthcare innovation.
Addressing Concerns of Losing Patient Connection with Virtual Care
As virtual care becomes a mainstay in healthcare delivery, a lingering concern remains: will this technology-driven approach reduce the personal connection between patients and providers? Market studies note that patients and providers feel virtual care offers significant convenience and benefits, but fear it risks feeling transactional when used in sensitive settings like inpatient care.
However, emerging data and real-world applications indicate that virtual care enhances—not diminishes—the patient experience, improving satisfaction, engagement, and continuity of care.
Evidence of Patient Satisfaction with Virtual Care
While concerns about depersonalization in healthcare delivery deserve careful consideration, a growing body of research challenges these assumptions. Multiple studies demonstrate that virtual care strengthens patient engagement and satisfaction:
A 2024 meta-analysis assessing patient satisfaction with telemedicine consultations offers evidence that patients generally exhibit high levels of satisfaction with the virtual model.
According to research from Statista, as of 2023, over half of patients surveyed in the United States indicated increased satisfaction with their care as a result of telemedicine.
Mayo Clinic research found that “quality metrics improved, along with significant improvement in patient satisfaction scores, as well as physician and support staff engagement and satisfaction” due to implementing advanced team-based care models that leverage in-room virtual care support.
After implementing a Virtual Nursing program, Florida-based Lee Health saw a 20% jump in patient satisfaction as reflected in HCAHPS scores as a result of enhancing the quality and immediacy of patient engagement. Patients report appreciating the availability of virtual nurses, who typically offer more focused interactions as they are less apt than bedside staff to be interrupted or juggling multiple tasks. “The personal nature of two-way video breaks through the glass,” said Lee Health’s System Director of Virtual Health and Telemedicine, Jon Witenko. “That human connection makes all the difference.”
A recent Becker’s Hospital Review article captures healthcare leaders’ sentiments that virtual care can enhance the overall patient experience by addressing bottlenecks in traditional workflows, “allowing nurses to have more time to engage meaningfully with patients.”
Collectively, the evidence highlights how virtual care drives better patient experience by fostering a sense of connectivity and attentiveness when implemented as part of a collaborative care model.
Virtual Acute Care’s Ripple Effect
Beyond direct patient interactions, virtual care offers additional benefits that indirectly improve patient satisfaction. One often-overlooked advantage is the boost in staff satisfaction. According to the American Association of Critical-Care Nurses (AACN), nurses in virtual care roles report feeling more fulfilled and supported, a factor that significantly enhances their interactions with patients. Happier, less overburdened nurses contribute to a more positive environment, creating a ripple effect of satisfaction that extends to patients.
Virtual care also facilitates greater patient-family engagement during inpatient stays. Relatives who may not be able to be physically present can join virtual consultations and discussions about care plans, promoting connection and involvement. This enhanced accessibility helps ease the emotional stress on patients and families, leading to greater overall satisfaction and outcomes.
Finally, virtual care solutions provide continuity of care that is difficult to achieve with in-person visits alone. For instance, remote engagement tools allow providers to track patients’ progress post-discharge, offering patients and families a reliable safety net. This level of oversight reassures patients, reducing anxiety about recovery and fostering a feeling of being genuinely cared for.
Embracing a Connected Future in Healthcare
As studies and real-world applications demonstrate, virtual care has tremendous potential to enhance, not hinder, the personal connection in healthcare. Improved patient satisfaction is one factor among a growing list of benefits leading health systems to implement virtual engagement at the hospital bedside. By integrating telehealth thoughtfully into clinical workflows, health systems can improve patient and family engagement and deliver a care experience that feels deeply connected and responsive.
Looking to enhance your patient communication and engagement strategy with virtual care? Schedule a call with one of our telehealth specialists today.
Trends from Becker’s, HLTH, and KLAS
Recent health conference conversations point to a new wave of priorities in healthcare technology. Over the past few weeks, Caregility executives attended Becker’s, HLTH, and KLAS events where AI and nurse enablement were repeatedly underscored as crucial factors in successful digital health transformation. The events provided valuable insights into how healthcare leaders are using technology to support clinical and operational goals, from addressing documentation burdens to building resilience against security risks. Here are some of our team’s key takeaways.
Mike Brandofino, President & COO Event: Becker’s 9th Annual Health IT + Digital Health + RCM Conference
“Telenursing was top of mind for a lot of folks at Becker’s. There were quite a few discussions about what virtual nursing programs can do and how to effectively deploy technology without negatively impacting bedside teams. Just throwing new technology at problems does not move the needle. Healthcare organizations are taking a more thoughtful approach to collaborative virtual care models.
There’s still a lot of confusion about what to do with AI. There’s concern about the validity of leveraging it in workflows in a way that saves time. The biggest item that healthcare providers are looking for is that documentation piece. Nurse notes, specifically. One session noted that the average nurse spends about four hours of their day documenting care. Many health systems are paying overtime hours for nurses to stay after their shift to do documentation. If health systems are going to get to better ratios, they’re going to need to fix that problem.”
Kedar Ganta, Chief Product & Engineering Officer Event: KLAS Digital Health Investment Symposium (DHIS) 2024
“Financial margin strains and cybersecurity threats dominated conversations at the KLAS DHIS event. There is growing recognition that navigating the next Black Swan event will require strong planning, governance, redundancies, operational resiliency, and investment in technology. Naturally, AI and cybersecurity repeatedly came up in discussions about building the resilience needed to withstand future disruptions. The recent events involving Change Healthcare and CrowdStrike heightened cybersecurity awareness across the industry. Organizations are actively developing playbooks to train for downtimes and implementing workarounds to ensure resiliency.
There is genuine interest and excitement about the potential of AI, but payer and provider attendees didn’t mince words about the challenges. There is little appetite for ‘black box’ AI and a strong call for greater transparency into what goes into AI. There is significant optimism about ambient speech technology for documentation. Most felt comfortable with the application of AI in revenue cycle management, patient communication, and imaging, but remained cautious about adoption in clinical workspaces.
Overall, there is a strong appetite for adopting technology that drives clinical efficiency and provides performance insights while ensuring security. Organizations are streamlining their tech stacks, prioritizing existing vendors, and leaning on their EHR vendors more to support clinical workflow optimization. Now more than ever, potential solutions are being evaluated through a monetary lens. Organizations recognize that virtual care is here to stay and are taking a strategic approach to broader implementation and governance.”
Jenna Walls, VP, Business Development & Strategic Alliances Event: HLTH 2024
“At HLTH, it was clear that AI is taking center stage in healthcare, but it’s important to note the shift in sentiment, particularly compared to just six months ago at ViVE. We’re seeing a more comfortable embrace of operational AI, but the industry remains cautious with clinical AI. That stance reflects our own approach to prioritizing responsible, incremental adoption and focusing on how AI enhances workflows rather than simply deploying new technology.
One of the standout discussions was around ambient scribing, but the conversation largely focused on relieving physicians’ burdens. We heard a strong call for similar support for nursing. It was great validation for what we’re addressing at Caregility. Our work with partners to create solutions that serve bedside teams—taking on tasks they don’t want to do or don’t have time to do—is where we see AI making the most positive impact.”
Lee Health Expands Virtual Nursing Program with Caregility
The Florida-based health system will significantly expand inpatient telehealth to connect hospital patients and staff with remote nurse resources.
Wall, NJ and Fort Myers, FL (Oct 16, 2024) – Lee Health, one of Florida’s largest health systems, is significantly expanding its Virtual Nursing Program with Caregility, a leading enterprise telehealth company.
Through the initiative, Lee Health continues its commitment to modernizing care delivery, enhancing clinical efficiency, and improving patient and staff satisfaction. The latest expansion includes the deployment of Caregility APS200 Duo dual-camera telehealth devices, building on the existing fleet of telehealth wall systems and carts to more than double the health system’s inpatient virtual care footprint. With this expansion, Lee Health’s virtual acute care infrastructure will cover more than half of the health system’s hospital beds, equipping nearly 1,000 patient rooms with bedside telehealth technology.
“The growth of our telehealth options accelerated during the COVID-19 pandemic out of necessity to ensure patients received important care safely and we were able to ensure continuous support for our medical teams,” said Rick Schooler, Chief Information Officer of Lee Health. “Through our expansion since then, we’ve evolved our virtual care capabilities to include an award-winning inpatient virtual observation program and now virtual nursing to improve patient outcomes utilizing available, improved technology to help our clinical staff.”
“This expansion is an important part of Lee Health’s broader strategy to modernize healthcare delivery,” said Jennifer Higgins, DNP, RN, NEA-BC, Chief Nursing Officer of Lee Health. “Our virtual nursing program introduces innovative possibilities in patient care workflows by connecting the care in the complex patient journey. From admissions and discharges to continuous patient monitoring, patients benefit from an additional team member dedicated to their care. We anticipate this additionally offering our nurses time for patients that need more hands-on care.”
“Having eyes and ears in every room enables remote caregivers to respond more effectively to the needs of patients and bedside staff across the enterprise,” said Wendy Deibert, Chief Nursing Officer at Caregility. “This expansion represents a significant step forward in Lee Health’s digital health strategy, paving the way for future innovation at the intersection of virtual care, bedside care, and AI, and we’re honored to support their mission to advance the art of what’s possible in healthcare delivery.”
As a foundational partner, Caregility has worked closely with Lee Health to create a future-proof solution that supports a broad array of clinical workflows, offers AI capabilities, and can support local edge processing. The Caregility Cloud™ virtual care platform serves as the backbone for all of Lee Health’s virtual care programs.
Lee Health’s investment scales its virtual nursing program, supported by Caregility’s unique remote fleet management tools, which mitigate device support hurdles and improve operations. With around-the-clock monitoring and support, as well as seamless software updates via Caregility’s cloud-based administration portal, Lee Health can ensure that its telehealth devices remain operational with minimal on-site maintenance requirements.
“With our edge-processing, dual-camera APS200 Duo devices that support multiple concurrent workflows, we have built a commercial offering designed to be deployed at scale,” said Ron Gaboury, CEO of Caregility. “Our mission with Lee Health and other customers is to set the foundation for long-term growth and hospital-room-of-the-future innovation. This empowers care teams to maximize virtual care workflows while reducing up-front costs and operational challenges associated with maintaining a device in every room.”
About Lee Health Since the opening of the first hospital in 1916, Lee Health has been a healthcare leader in Southwest Florida, constantly evolving to meet the needs of the community. A non-profit, integrated healthcare services organization, Lee Health is committed to the well-being of every individual served, focused on healthy living and maintaining good health. Healthcare services are conveniently located throughout the community in four acute care hospitals, two specialty hospitals, outpatient centers, walk-in medical centers, primary care and specialty physician practices, and other services across the continuum of care. Learn more at www.LeeHealth.org.
About Caregility Caregility (caregility.com) is a telehealth solution provider connecting care everywhere. Designated as the Best in KLAS® Virtual Care Platform (non-EMR) in 2021, 2022, and 2023, Caregility Cloud™ brings bedside care, virtual encounters, and AI capabilities together at the point of care. Doctors, nurses, and patients around the world rely on our intelligent telehealth edge devices and virtual nursing, observation, and engagement applications to enhance clinical insights, patient safety, and efficiency. Trusted by over 75 health systems, deployed in more than 1,000 hospitals, and supporting over 30,000 connected devices and millions of virtual sessions annually, Caregility is helping transform healthcare delivery across inpatient, outpatient, and home settings.
When evaluating AI solutions, it’s vital to ensure that technologies align with your healthcare organization’s needs and patient safety standards. As you navigate the complexities of AI integration, these questions are designed to help you thoughtfully evaluate tools.
Clinical Best Practices
How does the solution align with established clinical guidelines and standards of care?
How does the solution integrate with established clinical workflows and technologies?
What resources and training are provided to support operational resilience and user adoption?
What is the process for ensuring patient awareness and consent regarding the use of AI in their care?
Technical Best Practices
Can you explain how your AI models make decisions in a transparent, understandable way?
What testing processes are in place to validate that the AI’s decisions are sound?
How do you handle model updates or retraining to avoid clinical risks and disruption?
What are the infrastructure requirements to deploy the AI solution at scale?
Data Privacy and Security
Can you explain how your AI models make decisions in a transparent, understandable way?
What testing processes are in place to validate that the AI’s decisions are sound?
How do you handle model updates or retraining to avoid clinical risks and disruption?
What are the infrastructure requirements to deploy the AI solution at scale?
Return on Value
What is the total cost of ownership, including implementation, licensing, and support?
What are your plans for future development of this and other AI solutions?
Learn more
Set Up a Discovery Call
Caregility is here to help you implement a responsible Al strategy that enhances patient and staff experience while maintaining the highest care standards. Explore how our solutions seamlessly integrate with your existing workflows, safeguard patient data, and support your clinical teams.
When Virtual Nursing and AI Collide: Q&A with Mary Washington Healthcare
In our recent webinar When Virtual Nursing + AI Collide: Lessons from the Trenches, Mary Washinton Healthcare’s AVP of Hospital Operations Debra Marinari and Information Systems Analyst Trudy Osborne sat down with Caregility CNO Wendy Deibert to discuss their journey integrating remote nurses and artificial intelligence into inpatient care. Here are some key takeaways and practical strategies shared by our expert panelists.
1. How did you start your virtual nursing journey, and what were the initial challenges?
Mary Washington Healthcare began its virtual nursing journey a little over two years ago to modernize the health system’s approach to patient care. Reflecting on her 30-year nursing career, Marinari noted that many of the processes they used in the past would be considered outdated by today’s standards. She sees Virtual Nursing and AI as natural next steps in the health system’s journey to safer, more efficient patient care. One early challenge was getting experienced nurses to embrace the technology, but once they saw the benefits of improved support during staffing shortages, adoption quickly followed.
2. How is telehealth helping make care teams more agile?
Marinari and Osborne emphasized that telehealth has enhanced their ability to iterate quickly and uncover new opportunities for efficiency gains in nursing workflows. With a centralized Virtual Nursing hub on-site, remote nurses can triage and respond to inbound calls from the bedside, leaning on built-in backup coverage when multiple requests come in simultaneously. Mary Washington has seen improvements in nurse turnover rates and staff retention by implementing Virtual Nursing.
3. What workflows do Virtual Nursing and AI support?
In addition to supporting virtual admissions, discharges, and second signature verifications, virtual nurses also play a crucial role in supporting specialized workflows. For instance, virtual nurses can easily support MRI checklists and help determine the model of medical device (i.e. pacemakers) a patient has before procedures. The integration of Social Determinants of Health (SDOH) questionnaires into the virtual admissions process has increased completion rates to 98%, a dramatic improvement from before Virtual Nursing implementation. These workflows help ensure high-quality care and compliance.
4. How do you manage staffing and nurse-to-patient ratios for your Virtual Nursing program?
Mary Washington’s Virtual Nursing team is staffed with three virtual nurses per 12-hour shift, operating 24/7. The full-time roles were hired specifically for Virtual Nursing, with a minimum of two years of direct nursing experience required. Initially, the team was aligned by unit but later pivoted to a triage model that allows remote nurses to handle calls across multiple units as they come in. This flexibility has been key to managing staffing efficiently. The health system opted to add extra staffing support during peak hours when patient activity picks up between 11 am and 11 pm.
5. What platforms and AI tools are integrated with your Virtual Nursing program?
Osborne noted that the organization uses Epic for electronic health records, with virtual nurses leveraging secure chat within Epic to keep care teams connected. Mary Washington is in the process of integrating Critical Alert as their nurse call platform. Additionally, the organization is exploring health AI solutions like computer vision and ambient listening to assist with fall prevention and other early patient interventions. They are also lab-testing devices for contactless patient vital sign monitoring to improve early detection of patient deterioration and health issues.
6. How have Virtual Nursing and AI impacted patient care and staff efficiency?
One benefit of adding a remote nurse component to bedside care teams has been reduced documentation time, which has been a pain point for many nurses. By reassigning routine tasks, bedside nurses can focus more on direct patient care while remote nurses streamline workflows due to fewer interruptions. Although pilot programs are still in the early stages, the healthcare organization is excited about the promise of AI applications in areas like fall prevention and vital sign trending, which can further improve patient safety and nurse satisfaction.
7. Have patients or staff expressed concerns about virtual nursing or AI?
Marinari noted that patient resistance to Virtual Nursing has been minimal, with only one case involving a mental health patient who preferred in-person care. The staff’s attitude toward Virtual Nursing and AI has become increasingly positive, particularly as Mary Washington has fine-tuned its remote support processes over the last year. Marinari and Osborne actively work with nursing staff to continue to iterate and identify new workflows.
8. Are there specific metrics you’re tracking to measure success?
Since implementing Virtual Nursing, nurse satisfaction has improved significantly, and documentation time has decreased, both of which have been major wins for Mary Washington. The organization has also expanded its Virtual Nursing program into the emergency department and is actively tracking metrics related to nurse retention, patient outcomes, and fall rates to assess the program’s ongoing success.
9. What hardware supports your Virtual Nursing and AI implementation?
Dual-camera APS200 telehealth edge devices from Caregility, which include 40x zoom, far-end pan/tilt/zoom video capabilities, and night vision, are deployed in patient rooms to facilitate virtual nurse engagement. Bedside staff can press a vLert button to request remote nurse support. A minimalist, ceiling-mounted radar puck device supports contactless vitals capture. Osborne appreciates that deployment was straightforward, with centralized device management and strong vendor support throughout the process. The organization has also installed anti-ligature devices in the emergency department and is exploring facial scanning technology as a potential tool to support ED triage. The use of advanced hardware continues to evolve as the VN program expands.
10. What’s next for your Virtual Nursing and AI journey?
Looking ahead, Marinari expressed excitement about expanding AI capabilities, particularly in the area of computer vision for fall prevention. While the organization has made strides in reducing fall rates, this remains an area of focus, and they believe AI can further enhance early intervention. Additionally, the team is testing contactless devices that can provide early indicators of patient health trends, which they hope will lead to improved patient outcomes. They are also exploring new use cases in the emergency department and continue to work on integrating AI tools with existing platforms like Epic.
Do you have additional questions about Virtual Nursing and AI? Set up a discovery call to connect with our team of telehealth specialists and customer referral sites.
What’s New: Caregility September 2024 Update
Author: Kedar Ganta, Chief Product and Engineering Officer, Caregility
In my last post, I introduced our new family of dual-camera telehealth devices. Today, I want to share about additional workflow enhancements made possible through our ongoing platform innovation and integrations with new ecosystem partners.
iConsult
Our recent partnerships with Sonifi and Cyracom significantly enhance inpatient workflows with iConsult. Integration with Sonifi’s interactive patient engagement solutions offers patients a more comfortable and satisfying experience directly in their rooms. Meanwhile, Cyracom’s on-demand language interpretation services within iConsult effectively bridge language barriers and improve overall quality of care. iConsult now makes it easier to identify the location of patients using interpreter services, simplifying the internal billing process and improving overall efficiency.
iConsult P2P
In our outpatient iConsult P2P solution, the new polling feature enables group outpatient visits to become more dynamic and interactive. This allows healthcare teams to collect real-time feedback on patient needs, concerns, and preferences.
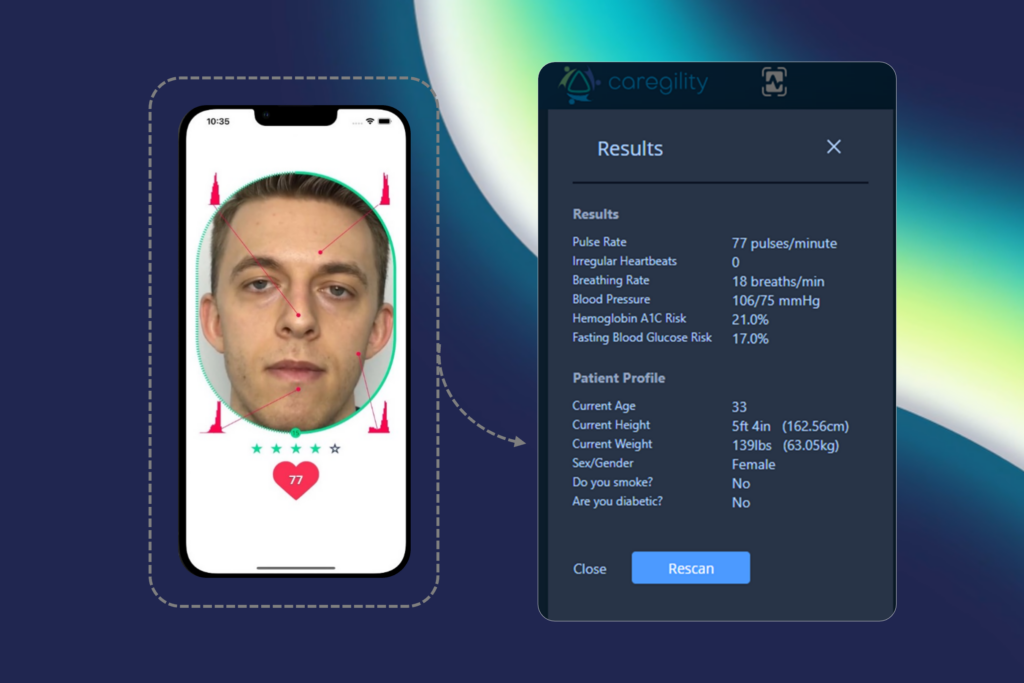
Also, don’t miss out on experiencing the AI-driven vitals scanning available within our P2P application. Using non-invasive computer vision technology, P2P analyzes a video stream of a patient’s face to measure vital signs such as heart rate, blood pressure, and respiratory rate.
iObserver
With the September 2024 release, iObserver has been enhanced with a new session transfer feature that maintains the same layout and patient tile location, providing a familiar and intuitive experience for virtual observers. These design improvements reduce cognitive overload and guide observers seamlessly through program list loading and session termination. Additionally, iObserver now provides insights into observer performance with metrics on virtual observer shift options, including intervention types and phrases.
Admin Portal
The success of your virtual care programs relies on visibility into your telehealth wall systems and carts. Our Admin Portal now serves as a command center, providing this visibility while facilitating fleet management. Admins can manage devices and perform soft reboots and seamless upgrades while filtering user accounts and devices by their associated programs.
Stay tuned for more updates as we continue to innovate and enhance workflows!



















 Clinical Best Practices
Clinical Best Practices

 Data Privacy and Security
Data Privacy and Security
 Return on Value
Return on Value